How Does a Telehealth Clinic Grow Its Women’s Hormone (HRT) Business? (The Symptom-Quiz Funnel and Why Women Want Meds, Not Supplements)
Most telehealth clinics that start with peptides and GLP-1s end up lopsided — the fast-moving weight-loss and peptide demand drowns out the higher-value hormone side of the business. One clinic we work with had it exactly backwards: about 70% of revenue from peptides and GLP-1s, only 30% from hormones, when the healthier mix is the reverse. Here is the FAQ on how a telehealth clinic actually grows its women’s hormone business — the symptom-quiz funnel that fills it, why menopause patients want medication and not another bag of supplements, and how diagnostic labs quietly turn peptide buyers into long-term hormone patients.
How does a telehealth clinic actually grow its women’s hormone (HRT) business?
Run a women’s-hormone ad into a symptom quiz that leads to a free discovery call — and offer the medications women actually want, not a functional supplement route.
Women are the most curious people on the internet and they love a quiz, so a “women’s hormone” or “menopause” ad that opens a short symptom quiz consistently outperforms a generic “book a consult” ad.
The quiz:
- Lowers the barrier
- Captures the lead
- Warms her up before a human ever talks to her
From there a free discovery call closes the relationship.
The mistake almost every competitor makes is what comes next. They draw a menopause crowd and then push a functional, supplement-first protocol — and the women bounce, because they came for relief and they want real treatment.
Build the funnel to deliver the meds the patient actually wants (estradiol, progesterone, low-dose testosterone, and where appropriate a GLP-1), and the same traffic that competitors waste converts for you.
Why do women’s hormone patients want medication, not just supplements?
Because they are already symptomatic, already dismissed once, and looking for something that actually works — not a wellness starter kit.
The women searching for hormone help are usually in or near menopause, have often been told their labs “look fine,” and have tried the soft stuff.
When a clinic answers that with another stack of supplements, it reads as one more brush-off.
We regularly absorb patients who paid thousands for a competitor’s functional program and walked away saying all they got was supplements.
Price was never the obstacle.
The obstacle was that nobody gave them the treatment they came for.
This is the whole positioning opportunity.
A clinic that offers real hormone therapy — clearly, confidently, and with proper labs behind it — beats the functional-only competitor on the exact patient that competitor spent money to attract.
You are not creating demand.
You are catching demand someone else is mishandling.
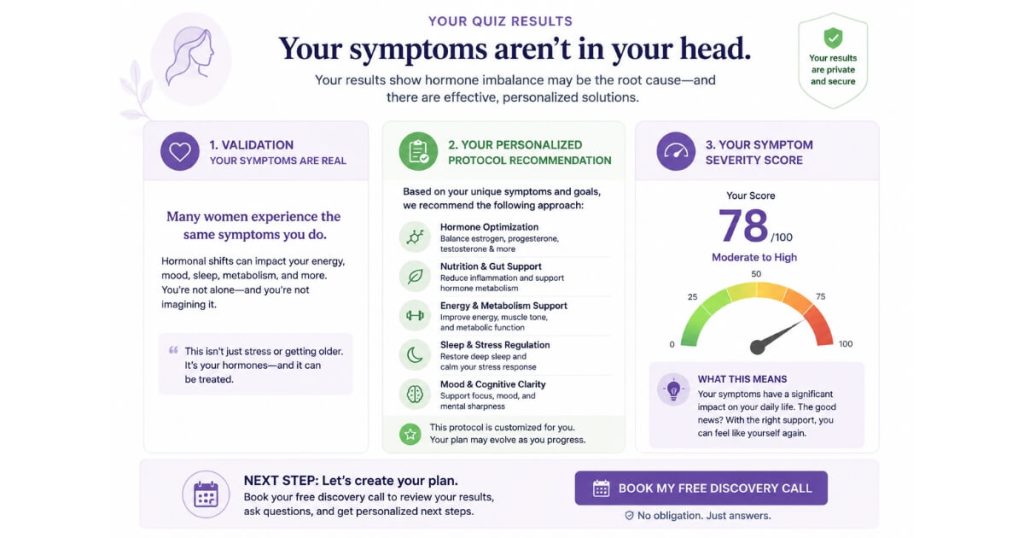
What should a women’s hormone symptom quiz actually do?
Three things:
- Validate that her symptoms are real.
- Output a personalized protocol recommendation.
- Give her a symptom-severity score so she gets an answer immediately.
The quiz is not a lead-capture gimmick — it is the first moment of care.
The opening reframe matters:
“Your symptoms aren’t in your head, and they’re not just menopause.”
That single line does more conversion work than any discount, because it speaks to a woman who has been dismissed by conventional care.
From there the quiz should return a personalized protocol recommendation (the specific hormones and, where relevant, a GLP-1) and a severity score so she feels seen, gets answers right away, and leaves with hope instead of another waitlist.
Even the leads who are not hormone-ready still convert.
A 28-year-old who fills out the quiz because she is gaining weight may not be a menopause patient, but she is a GLP-1 patient — so the funnel monetizes the full range of women who raise their hand.
We have watched this research-and-quiz behavior drive growth at Longevity & Functional Medicine Clinic Case Study, because the patients who self-educate before booking convert at a far higher rate.
How do I turn peptide and GLP-1 patients into higher-LTV hormone patients?
Use diagnostic labs as the bridge.
They make the case for hormone therapy without depending on a salesperson, and most peptide patients are closer to hormones than they realize.
Men who start a peptide like BPC-157 are often 9 to 12 months away from wanting TRT — they just do not know it yet.
The way to surface that is bloodwork.
Offer free or discounted labs to any patient who has already spent over a thousand dollars with you, then let a finding like low free testosterone make the argument.
Labs level the playing field: you are no longer relying on whether a given rep is a talented closer, because the deficiency sells the hormone program logically and on its own.
The same mechanic works on the women’s side.
A GLP-1 weight-loss patient who gets her hormones checked frequently discovers the real driver of her symptoms, and a peptide patient who feels better becomes a patient who stays for years.
This is exactly the cross-sell engine behind Eternity Health Partners Case Study — recurring hormone memberships, not one-off peptide cycles, are what build that kind of durable revenue.
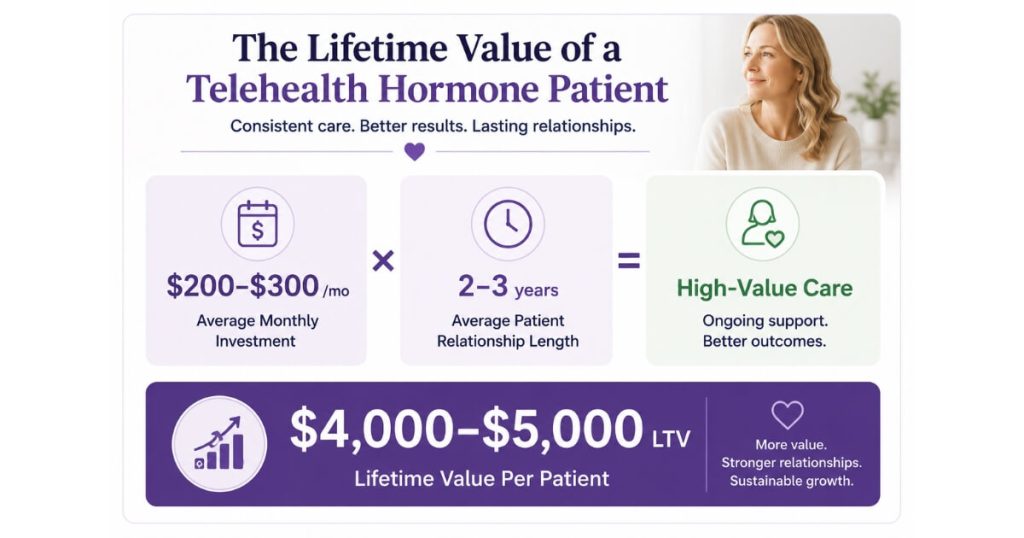
What’s the lifetime value of a telehealth hormone patient versus a peptide-only patient?
A telehealth hormone patient is worth roughly $4,000 to $5,000 in lifetime value — $200 to $300 a month for two to three years.
A peptide-only patient churns out at every cycle gap.
That LTV gap is the whole reason to flip a 70%-peptide / 30%-hormone revenue mix toward hormones.
Peptides run in cycles — commonly ten to twelve weeks on, then four weeks off — and patients drop off in that gap and again at each reorder.
Hormone patients, by contrast, stay on therapy for years because the result is something they do not want to lose.
One recurring hormone membership is worth many interrupted peptide cycles.
The high-ticket nature of that LTV is also why you cannot close it on automation alone.
A patient is not committing to $4,000–$5,000 of care from an email sequence.
You need either a human on a discovery call or diagnostic labs in the mix to carry the decision — and labs are the more scalable of the two, because they are logical and do not depend on a specific rep’s closing skill.
How much should I budget for women’s hormone ads, and when do I scale?
Start at about $75 a day, expect a three-week warm-up before the account performs, and move to Performance Max once a campaign reaches roughly $200 a day.
New ad accounts do not perform on day one.
Budget for a learning period of about three weeks before you judge the results, and resist the urge to kill a campaign mid-warm-up.
A comparable clinic:
- Spends around $120 a day
- Books scheduled discovery calls for roughly $150 each
These are useful benchmarks for what “working” looks like once the account is past warm-up.
When a search campaign reliably reaches about $200 a day, graduate it into Performance Max so YouTube and video assets start compounding.
The other quiet lever is the booking step itself: many telehealth clinics bleed leads because their EHR forces a clunky scheduling flow, so add a direct “book a discovery call” call-to-action and stop losing women who were ready to talk.
FAQ’s About This
Should a telehealth clinic offer supplements or medication for women’s hormones?
Lead with medication.
Women searching for hormone help are symptomatic and have usually been dismissed once already, so a supplement-first protocol reads as another brush-off.
Clinics that offer the hormones women actually want — with proper labs behind them — win the exact patient that supplement-only competitors paid to attract.
Does a symptom quiz really convert better than a “book a consult” ad?
Yes, for women’s hormones especially.
A quiz lowers the barrier, captures the lead, and validates her symptoms before a human talks to her.
The key is that the quiz returns a personalized protocol recommendation and a severity score, so she gets an answer immediately instead of just landing on a calendar.
How do I get peptide or GLP-1 patients to start hormone therapy?
Offer free or discounted labs to anyone who has already spent over $1,000 with you, then let the findings make the case.
Men on peptides are often 9 to 12 months from wanting TRT, and a low free-testosterone result sells the program logically — without depending on a salesperson’s skill.
What is a telehealth hormone patient actually worth?
Roughly $4,000 to $5,000 in lifetime value — about $200 to $300 a month sustained over two to three years.
That durability is why a hormone-heavy revenue mix beats a peptide-heavy one, since peptide patients churn at every cycle gap.
Why can’t I sell a high-ticket hormone membership with automation alone?
Because patients will not commit to several thousand dollars of care from an email sequence.
You need a human discovery call or diagnostic labs in the decision, and labs are the more scalable option because they make the case logically rather than depending on a closer.
What’s the next step?
If your telehealth clinic is heavy on peptides and GLP-1s and light on hormones, the fix is not more peptide ads.
It is a women’s-hormone funnel that:
- Validates real symptoms
- Offers the medication patients actually want
- Uses labs to bridge your existing buyers into long-term hormone memberships
That is how you flip the revenue mix toward the higher-LTV side of the business.
If you want someone to build that funnel with you — the quiz, the offer, the labs bridge, and the ad budget plan — that is the conversation to book.
We will map the path from a $75-a-day test to a hormone membership base on the call.