Should a Cash-Pay Clinic Add a DPC + HRT Subscription Model?
If your clinic is turning patients away because the schedule is booked out for weeks, you do not have a capacity problem—you have a payer problem. The constraint is rarely how many patients you can physically see. Instead, it is how many insurance-credentialed patients you can see. A direct primary care (DPC) plus HRT subscription model solves that problem by converting demand you cannot currently serve into predictable, recurring cash revenue. Better yet, it does so without forcing you to drop insurance. This guide explains when to add a DPC + HRT subscription, the recurring-revenue and retention math behind it, and how to launch it without overwhelming your team.
Should a cash-pay clinic add a DPC + HRT subscription model?
Yes.
If your clinic already has demand it cannot serve and you offer a recurring service such as HRT or peptides, a DPC + HRT subscription may be the highest-leverage offer you can add.
Why?
Because it monetizes the patients your insurance schedule is already turning away.
The biggest signal to watch is excess demand.
For example, are new patients waiting six to eight weeks for an appointment?
Is your cancellation list growing?
Are appointment requests consistently exceeding capacity?
If so, your challenge is not a lack of provider availability.
Instead, it is a lack of insurance-credentialed provider availability.
Credentialing a provider with major insurance carriers often takes around 60 days.
By contrast, a cash-pay provider typically only needs to be added to your malpractice coverage.
As a result, you can often place them on the schedule within a few weeks.
That means you can start serving patients much faster.
The subscription model simply wraps recurring revenue around that excess demand.
Instead of generating one-time cash visits, you create predictable monthly income.
HRT is particularly effective as the anchor.
Hormone therapy is naturally recurring.
Patients return month after month.
Consequently, the membership and the treatment reinforce each other.
Over time, that creates a stable revenue base that does not disappear when advertising pauses.
If you already have a nurse practitioner delivering hormone therapy, you can launch an HRT membership quickly and add peptide programs later.
For a broader look at how recurring cash offers fit into clinic growth, our guide to medical practice marketing explains how subscriptions fit into a larger growth strategy.
Do I have to drop insurance to add a DPC + HRT subscription?
No.
In fact, you should not.
The purpose of adding a DPC + HRT subscription is to complement your existing insurance business—not replace it.
Many clinic owners assume that moving toward cash-pay care means abandoning insurance.
That assumption often prevents them from acting.
However, the real bottleneck is not provider availability.
It is insurance-credentialed provider availability.
Because credentialing takes time, your schedule fills faster than you can expand insurance access.
A cash-pay provider solves that problem much more quickly.
You can add capacity, serve excess demand, and keep your insurance operations running exactly as they are.
Insurance continues generating revenue.
Meanwhile, recurring membership revenue grows underneath it.
Over time, this reduces dependence on insurance without requiring a sudden transition.
Think of it as a glide path rather than a cliff.
We worked with a practice where Dr. Groysman’s SGB clinic cut its insurance dependence in half by building cash-pay demand alongside its existing payer mix.
The DPC + HRT subscription follows the same strategy.
You grow recurring cash revenue until insurance becomes a choice rather than a necessity.

What should I charge for a DPC + HRT subscription?
Start by benchmarking local concierge medicine pricing.
Then provide more value than competing offers.
Finally, raise standalone visit pricing so the membership becomes the obvious choice.
For example, if a concierge physician in your market charges $3,000 annually, a $275-per-month subscription equals roughly $3,300 per year.
However, you can make the comparison far more compelling.
Bundle labs.
Offer discounts on hormones, peptides, and supplements.
Include sick visits for children.
In other words, make the membership solve multiple problems at once.
Patients are not simply paying for access.
They are paying to avoid surprise costs and recurring friction.
At the same time, maintain a fee-for-service option.
For example:
- $200 initial visit without labs
- $250 initial visit with labs
- $100 follow-up visit
This creates a pricing floor while positioning the membership as the better value.
Next, use what many operators call the “boiling pot” pricing strategy.
Launch at a price that attracts demand.
Measure how quickly appointments fill.
Then raise pricing every six weeks.
One clinic we worked with nearly doubled membership pricing from under $200 per month to $300–$350 per month, with and without hormones.
Despite the increases, they remained booked out for months.
Demand—not guesswork—revealed that pricing was too low.
What is the recurring-revenue and retention math on a subscription model?
The math is straightforward.
A subscription converts a one-time visit into recurring monthly revenue.
HRT strengthens that model because patients return consistently.
Consider a basic example.
One member paying $275 per month generates $3,300 annually.
One hundred members generate $330,000 annually.
That revenue can be forecast before the year even begins.
The leverage becomes even more obvious at scale.
Eternity Health Partners built to 250 members at $1,000 a month — $1.7M a year in recurring revenue.
That is what a mature subscription model can look like.
You do not need that exact pricing structure to benefit.
You simply need the recurring-revenue framework.
Predictable revenue changes how clinics hire.
It changes how they market.
It changes how they invest.
Most importantly, it creates stability.
Retention is where HRT becomes especially valuable.
Hormone therapy gives patients a clinical reason to remain engaged month after month.
As a result, churn remains lower than it is in many subscription businesses.
That dramatically improves lifetime value.
When patients stay for one or two years instead of a handful of visits, acquisition costs spread across thousands of dollars in revenue.
Each renewal becomes highly profitable.
Even better, many of these members are patients who otherwise would have remained on your waiting list.
That means the revenue is not just recurring—it is revenue you were previously losing altogether.
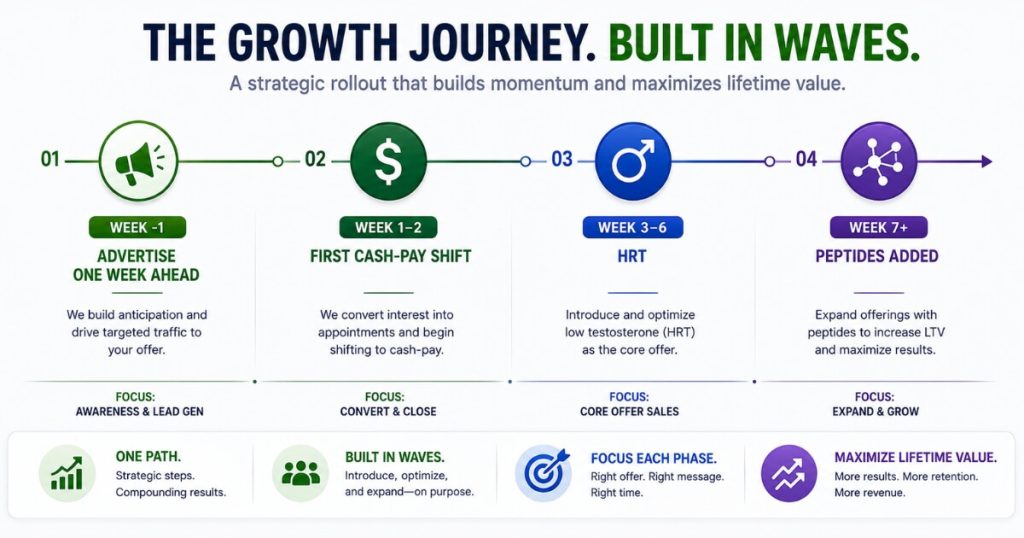
How do I launch a DPC + HRT subscription without overwhelming my staff?
Launch it with one provider.
Use dedicated cash-pay shifts.
Then roll out services in phases.
Start with a single cash-pay-only shift.
Ideally, use a provider who already wants additional hours.
Keep these shifts insurance-free.
Doing so gives you clean data on demand and performance.
Next, establish a clear launch date.
Your front desk needs time to prepare.
Scripts need to be written.
Handouts need to be created.
Pricing sheets need to be finalized.
Begin advertising roughly one week before launch.
That timing ensures inquiries arrive as the first appointments become available.
If demand is slow, the impact remains manageable.
If demand is strong, you can scale staffing accordingly.
Either way, the rest of the clinic continues operating normally.
Service sequencing matters too.
Launch DPC and HRT together first.
Most teams already understand hormone therapy workflows.
Once those processes are running smoothly, introduce peptides.
Avoid launching everything simultaneously.
The clinic that inspired this playbook scheduled front-desk training, pricing-sheet updates, HRT membership implementation, and peptide subscriptions in separate phases.
As a result, nothing fell through the cracks.
Treat the rollout as a controlled expansion rather than a dramatic switch.
That approach minimizes disruption while maximizing recurring revenue growth.
FAQ’s About Adding a DPC + HRT Subscription Model
Do I have to drop insurance to add a DPC + HRT subscription?
No. The subscription is designed to sit alongside your existing insurance business. Insurance keeps generating revenue while the membership program captures patients who do not want to wait six to eight weeks for an appointment. Over time, recurring cash revenue reduces dependence on insurance without requiring a sudden transition.
What should I charge for a DPC + HRT subscription?
Benchmark local concierge pricing and then offer more value. A $275-per-month membership can outperform a $3,000-per-year concierge model when it includes labs, discounts on hormones and supplements, and additional family benefits. Keep fee-for-service pricing available while positioning the membership as the stronger value proposition.
When does a DPC + HRT subscription actually make sense to add?
It makes sense when you already have excess patient demand and a recurring service such as HRT or peptides. The subscription does not create demand. Instead, it monetizes demand you already have while generating predictable recurring revenue.
How do I launch the subscription without overwhelming my staff?
Start with one provider and dedicated cash-pay shifts. Set a launch date, prepare front-desk scripts, advertise about a week before launch, and roll out services in phases. Launch DPC and HRT first, then add peptides later.
What does the front desk actually say so the subscription doesn’t feel like a hard sell?
Lead with insurance first. Explain the actual wait time. Then present the cash-pay option as a faster alternative. When patients understand the tradeoff, the membership feels like a solution rather than an upsell. Offer subscriptions only to patients who genuinely benefit from ongoing care and access.
What’s the next step?
If your clinic is turning away patients because insurance appointments are booked out for weeks, the opportunity is already sitting in front of you.
A DPC + HRT subscription transforms excess demand into recurring revenue.
It creates predictable cash flow.
It improves retention.
It reduces dependence on insurance over time.
Most importantly, it allows you to serve patients who would otherwise remain stuck on a waiting list.
If you want help designing the offer, pricing the membership, training the front desk, and building the rollout plan, that is the conversation to book.
We will map the subscription model and growth strategy for your clinic on the call.