How Do You Rebuild a Broken New-Patient Acquisition Model at a Cash-Pay Clinic?
The hardest acquisition problem to fix is the one that doesn’t look like a problem.
The phone is ringing. The ads are running. Leads are landing in the inbox.
And almost nobody signs up.
One cash-pay hormone clinic we sat down with was fielding roughly 190 inbound calls and converting 12 of them — and the owner’s instinct was to buy more leads.
That is the wrong move.
When motion isn’t turning into revenue, the model downstream of the lead is broken. Pouring more traffic into it just costs more money.
This is the rebuild — how to diagnose where a cash-pay clinic’s funnel actually leaks, and how to redesign the offer, the intake, and the close so prospects stop shopping and start signing up.
How do I know if my new-patient acquisition model is broken and not just my lead volume?
If leads are coming in but almost nobody signs up, you have a model problem, not a traffic problem.
The clearest signal is a wide gap between inbound interest and conversions.
The clinic we worked with kept circling back to the same number all call: 190 inbound calls a month, 12 signups.
“If we’re getting 190 inbound calls and only 12 people sign up,” the founding provider said, “it’s like, what’s going on?”
That is not the shape of a lead-volume problem.
A lead-volume problem looks like silence:
- Dead campaigns
- A cost per lead that won’t come down
- An empty calendar
A leak looks like the opposite: lots of activity, almost no revenue.
Motion without conversion.
So before you spend another dollar on ads, do the cheapest diagnostic there is.
Count the calls.
Count the signups.
Look at the ratio.
If the ratio is ugly, more leads will not fix it.
You will just pay to fill a bucket with a hole in the bottom.
The instinct to buy your way out of a conversion problem is the single most expensive mistake a cash-pay clinic makes, because it scales the leak.
Fixing the model first means every new lead you buy afterward is worth more.
This is the foundation of any serious patient acquisition system: the model has to convert before you feed it more volume.

Where do cash-pay clinic funnels actually leak?
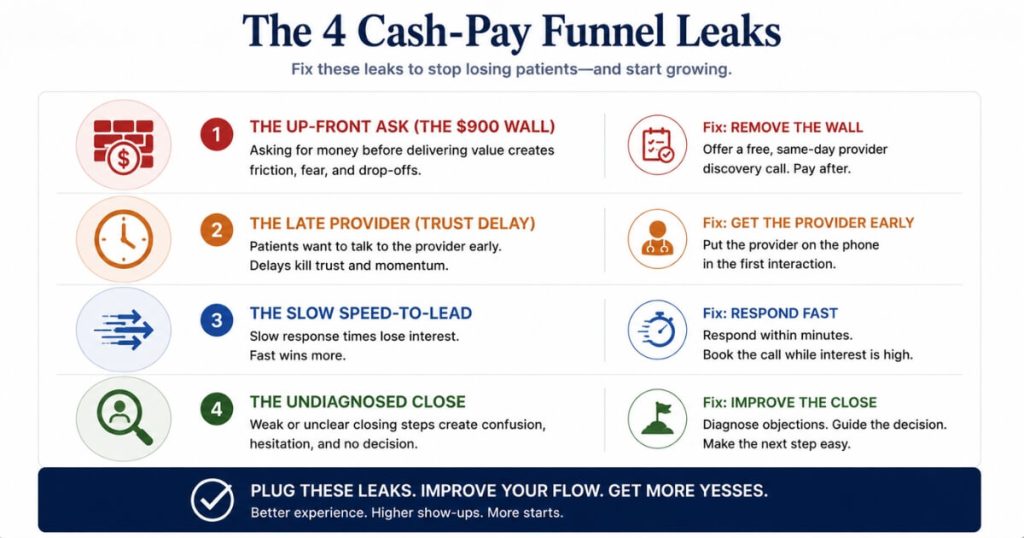
The four most common leaks are a too-big up-front ask, a provider who is gated too late, slow speed-to-lead, and an undiagnosed close.
The most expensive leak is usually the up-front ask.
At the clinic we worked with, prospects were asked for roughly $900 before they had ever met a provider — about $550 for labs and $350 for the consult.
“$900 is a big ask before they’ve even met us,” the founding provider said, paraphrasing the prospect’s own reaction:
“oh, it’s $900, give me your credit card — I don’t even know who you are.”
When the product is also available online, on a telehealth site, or from a guy reselling peptides at the gym, that wall sends shoppers straight to the cheaper option.
The second leak is sequencing.
The provider is gated too late.
If a prospect doesn’t talk to a clinician until deep in the process, there’s no rapport built when the credit card finally comes up.
The third leak is speed.
If a shopper has to wait days for a callback, they buy somewhere else first.
As we said on the call, “if they’re shopping, they’re shopping.”
The fourth is a quiet close problem.
The staff fielding calls aren’t converting, and nobody has watched the consults to find out why.
Most broken models run two or three of these at once.
That is exactly why a single fix rarely moves the number.
You patch one hole and the water keeps running out the others.
How do you redesign the offer when leads come in but won’t convert?
You lower the wall at the front door without lowering the price of the program.
The move is to separate the cost of getting started from the cost of being a member.
If you’re asking for hundreds of dollars in labs and consult fees before a prospect has met anyone, that up-front number is doing all the rejecting for you.
Credit the consult fee toward the first month so it stops feeling like a tax for showing up:
“if you sign up today, the consult fee goes toward your first month.”
You still make the money, because patients stay for months.
You just stop scaring off the ones who would have stayed.
The second half of the offer redesign is building an accessible entry path for shoppers who only want one thing.
A lot of inbound is now single-item demand:
- Someone wants a peptide
- Someone wants a GLP-1
- Someone wants a starter protocol
Forcing every one of them through a full hormone workup with a $550 lab panel collapses conversion.
Give them a fast, low-friction way in.
Then upsell into the full program once they trust you.
Critically, the recurring price is rarely the real objection.
A $395-per-month men’s program and a $425 women’s program convert fine.
It is the $900 wall in front of them that doesn’t.
Move the value forward.
Make the first step easy and cheap.
Then let the full program sell itself once trust exists.
What does speed-to-lead and a value-forward intake look like in a rebuilt model?
It looks like a same-day or next-day free 20-minute call with an actual provider, before any money changes hands.
The single biggest unlock in most rebuilds is moving the provider conversation forward.
Instead of one long 60-to-90-minute consult sitting behind a paywall, split it in two:
- A short meet-and-greet discovery call where a provider builds rapport and delivers real value
- A separate lab-review call later
“What you’re doing is you’re just moving the value forward, where previously they wouldn’t get this until much later — they got to talk to a doctor much sooner.”
That early, free, human contact is what converts a shopper into a patient.
The thing they’re actually buying at a cash-pay clinic is the relationship.
The mechanics matter.
The front office answers immediately and books the discovery call same-day or next-day.
“The big thing is speed here, because if they’re shopping, they’re shopping. If we can get them in same day or next day, this will do really well.”
The provider runs the call but does not take payment.
They hand the prospect back to the front office for checkout and intake.
That protects the provider’s positioning.
Clinicians are often uncomfortable asking for money mid-consult, and this keeps the rapport clean.
Value first.
Money second.
Then a live hand-off in between so nobody falls through the gap.
How do you fix the conversion and close problem instead of blaming the leads?
You record the consults, watch them, and find the holes — because you cannot fix a close you have never seen.
Owners reflexively blame leads or price.
But very often, the leads are fine and the close is leaking.
As the owner of that clinic put it, “I think membership close is a problem, not necessarily the leads — we’re still selling $900 bucks.”
The honest follow-up was that nobody actually knew why staff weren’t closing:
“there’s some holes there… we don’t know what that is yet.”
The fastest way to find out is to record or video the next week of initial consults.
Then watch where prospects drop.
You are hunting for the exact moment the energy dies:
- A flat pitch
- No offer presented
- No upsell
- No urgency
- A provider who never asks for the sale
Then you coach to those specific holes and rebuild the script around them.
One technique that reliably lifts close rate is choice-stacking.
Present three options at different price points and ask “which one do you want?”
That shifts the decision from yes-or-no to which-one.
This is the same conversion discipline that turned a clinic like Eternity Health Partners, which grew from $1M to $4M with 250 members, into a repeatable machine.
The leads only convert when the close behind them is dialed in.
And don’t change ten things at once.
Change one variable.
Watch the recordings.
Measure.
Then change the next.
That way, you can actually tell what moved the number instead of guessing.
How do you sequence the rebuild so you don’t kill what’s already working?
Run the new model as a 60-day pilot, change one or two things at a time, and keep a revert path.
A broken acquisition model almost always has a few things going right underneath it:
- A brand
- A reputation
- A core of loyal patients
A panicked overhaul can break those too.
So treat the rebuild as a controlled experiment.
Pick the two highest-leverage tweaks first:
- The fast, free discovery call with a provider
- The credited consult fee that lowers the entry wall
Run them for 60 days.
Measure conversion against your old baseline.
If it works, keep it and stack the next change.
A 60-day follow-up that upsells entry patients into the full membership is a natural second move.
By then, you can show them their own lab values and explain exactly why the full program is worth it.
If a change doesn’t work, you revert it.
You lost a pilot, not the business.
That discipline is what separates clinics that scale demand from clinics that thrash.
When the model is sound, more volume compounds.
It’s the same pattern behind a longevity and functional-medicine clinic that saw a 900% lead increase once the funnel underneath the leads could actually convert.
Move the value forward.
Lower the entry wall.
Watch the close.
Run it as a pilot.
Then let the data — not the panic — tell you which change to keep.
FAQ’s About Rebuilding a Patient Acquisition Model
How do I know if my new-patient acquisition model is broken and not just my lead volume?
If leads are coming in but almost nobody signs up, you have a model problem, not a traffic problem.
The clearest signal is a wide gap between inbound interest and conversions.
One clinic we worked with was fielding roughly 190 inbound calls a month and signing up only 12 people.
When the phone is ringing, the model downstream of the ring is the thing that is broken:
- The offer
- The speed of follow-up
- Who the prospect talks to first
- How money gets asked for
Lead volume problems look different.
They look like silence, dead campaigns, or a cost per lead that won’t come down.
A leak shows up as motion without revenue.
Before you spend a dollar more on ads, count the calls, count the signups, and look at the ratio.
If the ratio is ugly, more leads will not fix it.
You will just be paying to fill a bucket with a hole in the bottom.
Where do cash-pay clinic funnels actually leak?
The four most common leaks are a too-big up-front ask, a provider who is gated too late, slow speed-to-lead, and an undiagnosed close.
The most expensive one is usually the up-front ask.
At one cash-pay hormone clinic, prospects were asked for roughly $900 before they had ever met a provider.
That was about $550 for labs and $350 for a consult.
As the founding provider put it, “$900 is a big ask before they’ve even met us.”
The second leak is sequencing.
Prospects don’t talk to a provider until deep in the process, so there is no rapport when the credit card comes up.
The third is speed.
If a shopper has to wait days for a callback, they buy peptides or TRT online before you ever reach them.
The fourth is a quiet close problem.
The staff taking the calls aren’t converting, and nobody has watched the consults to find out why.
Most broken models have at least two of these leaks running at once.
That is why a single fix rarely moves the number.
How do you redesign the offer when leads come in but won’t convert at a cash-pay clinic?
You lower the wall at the front door without lowering the price of the program.
The move is to separate the cost of getting started from the cost of being a member.
If you are asking for hundreds of dollars in labs and consult fees before a prospect has met anyone, credit that consult fee toward the first month.
That way, it stops feeling like a tax for showing up.
Then build an accessible entry path for the shoppers who only want one thing:
- A peptide
- A GLP-1
- A starter protocol
Do not force everyone through the full hormone workup.
The recurring membership price is rarely the real objection.
A $395-per-month men’s program and a $425 women’s program convert fine when the entry experience makes sense.
It is the $900 wall before any value that kills the signup.
Move the value forward.
Make the first step easy and cheap.
Then let the full program reveal itself once trust exists.
What does speed-to-lead and a value-forward intake look like in a rebuilt model?
It looks like a same-day or next-day free 20-minute call with an actual provider, before any money changes hands.
The single biggest unlock in most rebuilds is moving the provider conversation forward.
Instead of one long 60-to-90-minute consult that sits behind a paywall, split it:
- A short meet-and-greet discovery call where a provider builds rapport and delivers real value
- A separate lab-review call later
The front office answers immediately and books the discovery call same-day or next-day.
Speed is the whole game.
As we put it on the call, “if they’re shopping, they’re shopping.”
Getting them in front of a provider same day is what wins them before a competitor does.
The provider runs the call but does not take payment.
They hand the prospect back to the front office for checkout.
That protects the provider’s positioning and keeps the rapport intact.
Value first.
Money second.
How do you fix the conversion and close problem instead of just blaming the leads?
You record the consults, watch them, and find the holes — because you cannot fix a close you have never seen.
Owners love to blame leads or price.
But very often, the leads are fine and the close is leaking.
The fastest diagnostic is to record or video the next week of initial consults and watch where prospects drop.
You are looking for the moment the energy dies:
- A flat pitch
- No offer presented
- No upsell
- No urgency
- A provider uncomfortable asking for money
Then you coach to those holes and rebuild the script around them.
One technique that consistently lifts close rate is choice-stacking.
Present three options at different price points and ask “which one do you want?”
That shifts the decision from yes-or-no to which-one.
And don’t change ten things at once.
Change one variable.
Watch the recordings.
Measure.
Then change the next.
That way, you actually learn what moved the number.
How do you sequence the rebuild so you don’t kill what’s already working?
Run the new model as a 60-day pilot, change one or two things at a time, and keep a revert path.
A broken acquisition model still has a few things going right:
- A brand
- A reputation
- A core of loyal patients
A panicked overhaul can break those too.
So treat the rebuild like a controlled experiment.
Pick the two highest-leverage tweaks:
- The easy, fast, free discovery call
- The credited consult fee
Run them for 60 days.
Measure conversion against your old baseline.
If it works, keep it and stack the next change.
That could be a 60-day follow-up to upsell entry patients into the full membership.
If it doesn’t, you revert.
You lost a pilot, not the business.
Depth and discipline beat a frantic rebuild.
Move the value forward.
Lower the entry wall.
Watch the close.
Then let the data tell you which change to keep.