What Is the Real ADvice 4 R’s Framework for Cash-Pay Medical Practice Teams? (Role, Responsibilities, Requirements, Results)
Most cash-pay medical practice owners we talk to are quietly frustrated with their teams. The team seems reluctant to make changes, productivity is uneven, and the owner ends up doing work that should have been delegated months ago. It’s almost never a hiring problem. It’s a documentation problem. The team was thrown into place without a written description of what each person actually owns — and you can’t hold someone accountable to a job that was never written down. The 4 R’s framework is the fix.
What is the Real ADvice 4 R’s framework?
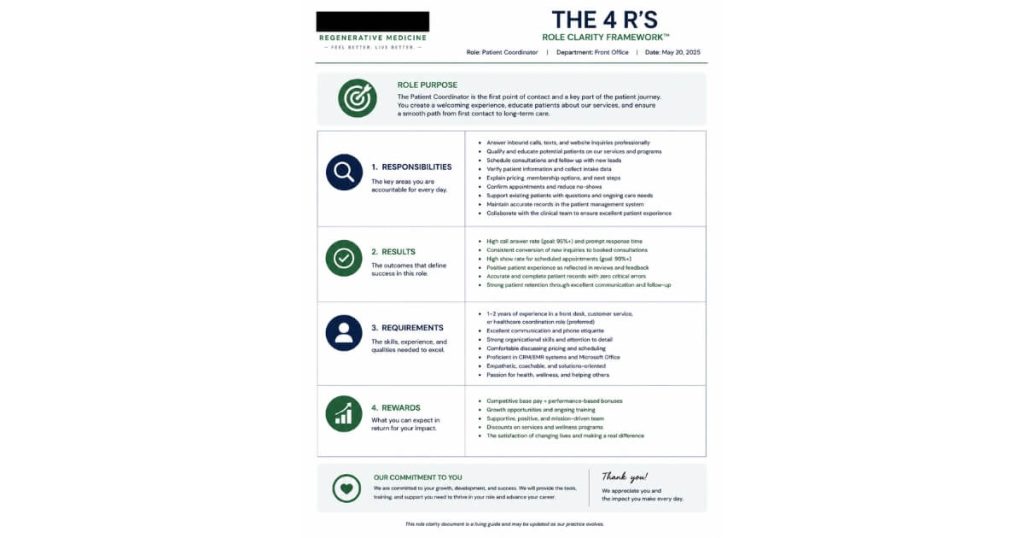
The 4 R’s framework is a one-page operational document Real ADvice creates for every position at a cash-pay medical practice — Role, Responsibilities, Requirements, and Results — so that every team member knows exactly what they own, how they’re measured, and what “good” looks like in their seat.
It exists because most clinic owners hire a great front desk lead, a great patient coordinator, or a great office manager, and then never write down what that person is solely responsible for.
The team member fills in the gaps with their best guess.
The owner fills in the rest with their own time.
Six months later the owner is frustrated that the team isn’t moving fast enough, and the team is frustrated that the owner keeps changing what “the job” means.
The 4 R’s document removes both problems by forcing the conversation onto paper before the hire, not after the frustration.
- Four columns
- One page per role
- Updated quarterly
That’s the whole framework.
What does each of the 4 R’s actually mean?
Role
Role is the position title and the one-sentence description of why this role exists at the clinic.
Most clinics already have job titles.
The trap is the description.
“Patient Coordinator”
…doesn’t tell anyone what the role actually does.
“Owns the conversion of every new inquiry into a paid first appointment, and the attendance rate on those appointments”
…does.
Two sentences max.
The role description is the answer to:
“Why is this seat at the clinic?”
Responsibilities
Responsibilities is the bulleted list of tasks and processes this person owns end-to-end — not “helps with,” not “supports” — owns.
This is where most clinics break.
The owner thinks the front desk owns lead follow-up, the front desk thinks the owner reviews leads in the morning, and leads sit in the CRM for three days.
A real Responsibilities list reads like a process flow:
“Within 5 minutes of any new website inquiry, dial the lead twice, leave a voicemail, send an SMS, send a calendar link.”
That level of specificity is the whole point.
If two people read the Responsibilities list and disagree on what’s expected, the document isn’t done.
Requirements
Requirements is the systems, training, and standards this person must follow to execute the responsibilities.
It’s the CRM they use, the script they read, the SOP they follow, the standards they’re held to.
Example:
“Patient Coordinator must use the GHL pipeline, follow the inbound call script verbatim, and log every call disposition before end of day.”
This is the column that prevents the team from inventing their own workflow when something breaks.
Results
Results is the numeric outcomes this person is measured on weekly and monthly.
This is the column most owners avoid because it requires picking numbers.
Don’t avoid it.
Pick three to five metrics per role.
Example metrics by role:
Patient Coordinator
- Cost per scheduled appointment
- Attendance rate on scheduled appointments
- Conversion rate from attended consult to paid first treatment
Marketing Lead
- Cost per lead
- Lead-to-appointment rate
- Return on ad spend by channel
Office Manager
- Payroll-as-percent-of-revenue
- Vendor cost trend
- Weekly KPI report shipped on time
When Results are written down, the weekly numbers review writes itself.
Why do most cash-pay medical practice teams underperform without a 4 R’s document?
Because the team doesn’t know what they’re supposed to be doing, and the owner doesn’t know what systems the team has cobbled together to make things work.
When someone is hired without a 4 R’s document, they import whatever process they ran at their last job — or they invent one.
The owner doesn’t see the system because it’s in the team member’s head and on a few Post-it notes around the front desk.
Six months in, the team member quits, gets sick, or goes on vacation, and the clinic discovers that 30% of the operation lived in one person’s notebook.
- Inbound calls don’t get returned
- Lab work doesn’t get ordered
- The provider walks into a consult cold because the prep sheet was never built into a repeatable system
Without the document, you also can’t fairly hold the team accountable.
The first time the owner says:
“You should have followed up on that lead within the hour”
…the team member can correctly say:
“No one told me that was the rule.”
With the 4 R’s doc, the rule is written down, the team member signed off on it the day they were hired, and the accountability conversation is short and direct.
The document doesn’t make people better at their job — it makes the standard explicit so that good people can hit it and underperformers self-select out.
In what order should I write 4 R’s documents for my cash-pay medical practice?
In hiring order:
- Office Manager
- Patient Coordinator
- Marketing Lead
- Clinical Director
Document the role you’re about to hire before you make the offer, not after the new hire is sitting in the chair.
Office Manager first
Because the role exists to free the owner’s calendar.
If you can’t write down what the Office Manager owns, you don’t have a job to hire for — you have a wish.
Patient Coordinator second
Because that role owns the revenue from new patient acquisition.
Marketing Lead third
Because by the time you hire one, the operational base is solid enough that paid spend actually converts.
Clinical Director last
Because a clinical hire inherits the operational machine you’ve already built.
Every position had a 4 R’s doc before the offer letter went out.
The order matters because every role above the Office Manager generates more work that ultimately routes to the owner unless the operational base is in place.
- Hire the Marketing Lead first and ad spend climbs while conversion doesn’t
- Hire the Clinical Director first and now you’ve added another provider to a practice that still funnels every operational decision through one person
How often should a cash-pay clinic update its 4 R’s documents?
Quarterly at minimum, and any time the role changes meaningfully:
- New software
- New process
- New metric
- New commission structure
Quarterly is the cadence because cash-pay clinics evolve fast.
Six months ago the Patient Coordinator wasn’t following a script for GLP-1 cross-sells. Now they should be.
Six months ago the Office Manager wasn’t running the weekly KPI report. Now they own it.
If the document doesn’t reflect the actual job, the team starts ignoring it and the framework collapses back into Post-it notes.
The owner doesn’t write the updated 4 R’s alone.
The team member in the seat drafts the update first — they know the job better than anyone.
The owner reviews, edits the Results column to keep the metric standards tight, and both parties sign the updated version.
- The team member keeps a copy
- A master copy lives in the operations folder
The act of updating the document is itself the quarterly accountability conversation:
“Here’s what we agreed you own; how are we doing on each line?”
Done correctly, the 4 R’s review takes 30 minutes per role, four times a year.
That’s two hours of owner time per role per year — the cheapest accountability infrastructure a cash-pay practice will ever buy.
Can the 4 R’s framework work at a smaller cash-pay clinic with only two or three team members?
Yes — and arguably it matters more at a small clinic than a large one, because at a small clinic every dropped responsibility lands directly on the owner.
A two-person clinic where:
- The owner-provider also runs marketing
- The front desk person handles inbound calls, scheduling, and intake
…needs 4 R’s documents more than a 20-person clinic does.
Without them, when the front desk person calls in sick, the owner is suddenly back at the front desk fielding calls instead of seeing patients.
With them, the role is defined tightly enough that:
- A temp
- A virtual receptionist
- A part-time hire
…can read the doc and execute 80% of the job from day one.
That kind of scale starts at a two-person practice.
It doesn’t start once the team is already large.
What’s the next step?
If your cash-pay medical practice has more than one team member and you don’t have a 4 R’s document for each role, that’s the highest-leverage fix you can make this quarter.
Book a strategy call with Real ADvice.
In 60 minutes we’ll:
- Map which role at your clinic needs a 4 R’s doc first
- Walk through the four columns for your specific practice
- Show you the exact templates we’ve used with HRT, functional medicine, regenerative pain, and GLP-1 clinics
If it’s a fit, we’ll build them with your team over 90 days.