What Should a Patient-Acquisition Phone Script for Weight-Loss and DPC Sound Like?
Most cash-pay clinics lose patients on the phone, not in the ad.
The leads come in — weight-loss, hormone, direct primary care — and then they hit a front desk that quotes a price it cannot legally quote, dodges the close, and lets the lead hang up without an appointment.
This is the script that fixes that: the inbound and outbound call flow for weight-loss and DPC patient acquisition.
It covers how fast to call back, what to ask, how to handle “how much,” how to book with a card on file, and how to make sure no call ends without a next step.
The ads create the lead.
The phone is where the patient acquisition actually happens.
How fast should a cash-pay clinic call back a weight-loss or DPC lead?
Inside five minutes for a fresh inbound lead.
Same business day at the latest for any form fill or missed call.
Speed-to-lead is the single biggest lever on a cash-pay clinic’s booking rate.
A weight-loss or DPC lead is comparison-shopping in real time.
They filled out three forms, not one.
The clinic that calls first usually books the appointment.
The lead who picks up in the first few minutes is still emotionally in the decision.
The lead you call back two days later has already moved on.
This is the part of patient acquisition for cash-pay clinics that no ad budget can fix.
If the phone does not get answered and the missed leads do not get called back the same hour, the spend leaks out the bottom.
Build the outbound script to assume the lead barely remembers filling out the form.
The opener that works is low-pressure and specific:
“Hi, is this ___? This is Sara with the clinic. I saw you hadn’t scheduled your free provider consultation yet, so I wanted to reach out. Would it be easier if I just helped you schedule with one of our providers over the phone?”
If they do not answer, leave a real voicemail naming the offer.
Then follow with a text.
The text often earns the callback the voicemail set up.

What discovery questions should the script ask a weight-loss lead before booking?
Ask whether they have tried weight-loss injections before.
Then ask what happened last time, how many pounds they want to lose, and why now.
Use that order.
The point of discovery is not to qualify the lead out.
It is to make them feel understood.
It also gathers the information the booking form needs anyway.
Start with:
“Have you tried weight-loss injections before, or would this be your first time?”
If they have, follow with:
“What were you taking and roughly what dose?”
Then ask:
“What happened last time that made you stop?”
Then:
“About how many pounds are you looking to lose?”
Each answer is one fewer question on the booking form later.
Discovery and data capture become the same motion.
The highest-converting question in the entire script is the one about motivation:
“Do you have any events coming up, or anything making losing this weight a priority for you right now?”
That surfaces the emotional driver.
It might be:
- A wedding
- A reunion
- A doctor’s warning
It also gives the rep the moment to empathize before moving on.
A simple “That makes sense” does more for the close than any feature pitch.
People do not book a clinic that interviews them.
They book the one that listens.
Discovery is where trust is built.
Trust is what carries the lead through the price question that comes next.
What should the script say when a weight-loss caller asks “how much does it cost?”
Acknowledge the question.
Explain that price depends on the dose and medication the provider recommends.
Then redirect to the complimentary discovery call where they get a real number.
This is the moment most front desks blow the call.
They either guess a number that scares the lead off, or they stammer and lose credibility.
The framing that works is honest and patient-centered:
“I totally get that. Our pricing is based on the dose and the specific medication, and because I’m not a medical provider it’s actually unsafe for me to guess on a dose or price without the provider reviewing your situation. The good news is that discovery call is complimentary — the provider will tell you what they recommend and give you precise pricing options before you decide anything.”
This is not a dodge.
Patients accept it because it is framed around their safety, not the clinic’s reluctance to quote.
You can offer a floor to relieve sticker anxiety:
“We have programs starting as low as $200, depending on the dosage the provider recommends.”
But never give a ceiling.
Never guess.
The rule is simple:
The price objection always ends with a scheduling question, not a number.
Use:
“So the fastest way to get a real number is to get you on that free call. What day works better for you, early or later in the week?”
The objection becomes the bridge to the booking.
How does the booking step work, and why take a card on file for a free consultation?
Assume the close.
Offer two time choices.
Take a card on file to reserve the slot.
Explain that it is zero dollars today and only used if they no-show without notice.
The card-on-file step is what separates a real booking from a tire-kicker.
It is the single most important mechanic in the script.
Do not ask:
“Do you want to book?”
That invites a no.
Assume the close and offer a choice between two yeses:
“What day works best — early in the week or later? Morning or afternoon?”
Once they pick, lock it immediately:
“Great, I’ve got Tuesday at 2 with the provider. To hold that slot, what kind of card do you want to use — Visa or Mastercard?”
Frame the card honestly every time:
“It’s zero dollars today; it only gets used if you no-show without letting us know.”
That framing protects the clinic’s calendar from the no-show rate that quietly kills free-consult funnels.
It also raises the quality of who shows up.
A lead willing to put a card down to hold a free call is a lead who intends to come.
Collect the rest of the booking details using what you already gathered in discovery.
That way, the patient never answers the same question twice.
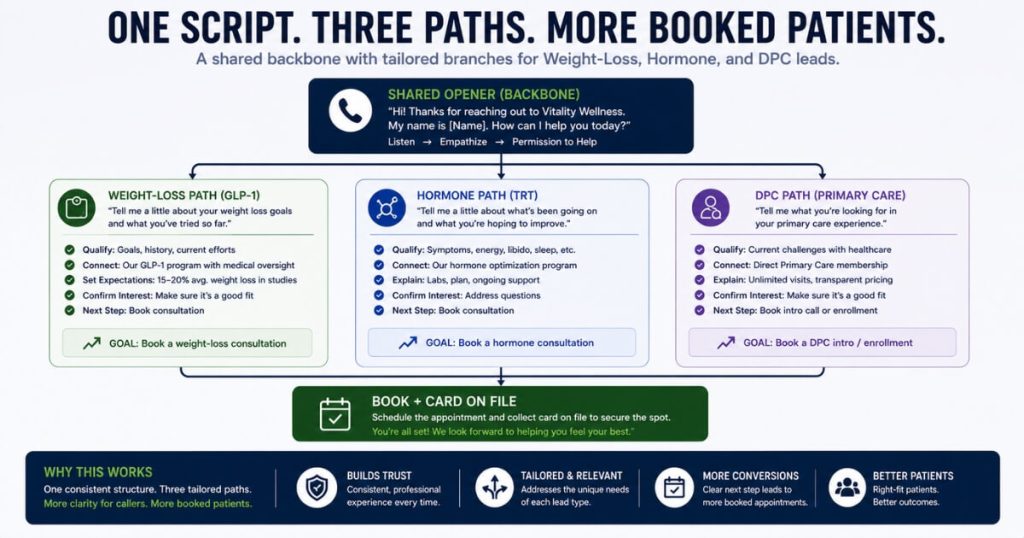
How should the script change for hormone and DPC leads versus weight-loss leads?
Keep the same backbone:
- Speed
- Discovery
- Permission
- Book
- Card
Then swap the offer structure to match how each program is sold.
The opening is universal:
“Thank you for calling, this is ___. Who am I speaking with? How can we help you today?”
If the caller does not volunteer, the rep offers the menu:
“Are you calling about weight-loss injections, hormones, or primary care?”
Then the rep jumps to the right branch.
Weight-loss runs on a free discovery call held by a card.
Hormone runs on a paid labs-plus-review structure:
“Step one is labs — three hundred dollars for a comprehensive panel so the provider isn’t guessing. Step two is the review visit, also three hundred dollars, and if you start the membership that fee is credited toward your first month.”
Direct primary care and ADHD lead with the membership:
“You enroll first, then your initial consult covers meds, refills, and your treatment plan, and ongoing access is included.”
The discovery questions shift too.
For hormone and DPC, the rep asks:
- Whether they have a current provider
- Why they are switching
- What they are not getting now
But the permission-to-explain beat stays the same.
The assume-the-close booking stays the same.
The card on file stays the same.
That is why one script with three branches is far easier to train than three separate ones.
To see how this phone layer fits into a full acquisition system, the Eternity Health Partners build that produced 60 new patient inbound calls a month shows ads and phone working as one machine.
How do you make sure no patient-acquisition call ends without a booked next step?
Make “no call ends without a scheduled next step” the rule the script is built around.
Then give the rep a fallback for the lead who will not book today.
The default outcome of every call is a booked appointment with a card on file.
But the script has to plan for the lead who genuinely will not commit.
Hanging up and hoping they come back loses the lead you already paid to generate.
The fallback is a text capture:
“Totally fine. If it’s okay with you, I’ll text you our scheduling link so when you’re ready you can grab a spot before they fill up. What’s the best cell number to use?”
That pulls the lead into a follow-up sequence instead of letting them evaporate.
It does this without pressure.
Put it all together and the script is a system:
- Same-day callback
- Discovery conversation that builds trust
- Price objection that ends in a scheduling question
- Card-on-file booking that protects the calendar
- Never-end-without-a-next-step rule
That is what turns ad spend into booked patients.
We have seen the same phone discipline compound at scale.
A weight-loss and medspa clinic where front-end demand plus a tight booking operation drove 3,727 new patients in a single year at NuLevel Wellness.
The phone script is where the patient acquisition actually happens.
FAQ’s About Weight-Loss and DPC Patient-Acquisition Scripts
How fast should a cash-pay clinic call back a weight-loss or DPC lead?
Inside five minutes for a fresh inbound lead.
Same business day at the latest for any form fill or missed call.
Speed-to-lead is the single biggest lever on a cash-pay clinic’s booking rate.
A weight-loss or DPC lead is comparison-shopping in real time.
They filled out three forms, not one.
The clinic that calls first usually books the appointment.
The lead who picks up the phone in the first few minutes is still emotionally in the decision.
The lead you call back two days later has already moved on or booked elsewhere.
Build the outbound script to assume the lead barely remembers filling out the form:
“Hi, is this ___? This is Sara with the clinic. I had a few minutes and saw you hadn’t scheduled your free provider consultation yet, so I wanted to reach out.”
Leave a real voicemail if they do not answer.
Then follow with a text.
The text often gets the callback the voicemail earns.
The clinics that win patient acquisition are not the ones with the best ad.
They are the ones whose phone gets answered and whose missed leads get called back the same hour.
What discovery questions should the script ask a weight-loss lead before booking?
Ask whether they have tried weight-loss injections before.
Then ask what happened last time, how many pounds they want to lose, and why now.
Use that order.
The point of discovery is not to qualify the lead out.
It is to make them feel understood and collect the information the booking form needs anyway.
Start with:
“Have you tried weight-loss injections before, or would this be your first time?”
If they have, ask:
“Do you remember what you were taking and roughly what dose?”
Then:
“What happened last time that made you stop?”
Then:
“About how many pounds are you looking to lose?”
Finally, ask the highest-converting question:
“Do you have any events coming up, or anything making losing this weight a priority for you right now?”
That last question surfaces the emotional driver.
The rep’s job is to empathize before moving on.
Every answer collected here is one fewer question on the booking form.
Discovery and data capture become the same motion.
What should the script say when a weight-loss caller asks “how much does it cost?”
Acknowledge the question.
Explain that price depends on the dose and medication the provider recommends.
Then redirect to the complimentary discovery call where they get a real number.
Use this framing:
“I totally get that. Our pricing is based on the dose and the specific medication, and because I’m not a medical provider it’s actually unsafe for me to guess on a dose or price without the provider reviewing your situation. The good news is that discovery call is complimentary — the provider will tell you what they recommend, go over exact dosing, and give you precise pricing options before you decide anything.”
This is not a dodge.
It is framed around patient safety.
You can give a floor to relieve sticker anxiety:
“We have programs starting as low as $200, depending on the dosage the provider recommends.”
But never give a ceiling.
Never guess.
The fastest way to get a real number is to get them on the free call.
So the price objection should always end with a scheduling question, not a number.
How does the booking step work, and why take a card on file for a free consultation?
Assume the close.
Offer two time choices.
Take a card on file to reserve the slot.
Explain that it is zero dollars today and only used if they no-show without notice.
Do not ask:
“Do you want to book?”
Ask:
“What day usually works best for you — early in the week or later? Morning or afternoon?”
Once they pick, lock it:
“Great, I’ve got Tuesday at 2 with the provider. To hold that slot, what kind of card do you want to use to reserve your discovery call — Visa or Mastercard?”
Frame the card honestly:
“It’s zero dollars today; it only gets used if you no-show without letting us know.”
That protects the clinic’s calendar.
It also raises the quality of who shows up.
A lead willing to put a card down to hold a free call is a lead who intends to come.
How should the script change for hormone and DPC leads versus weight-loss leads?
Keep the same backbone:
- Speed
- Discovery
- Permission
- Book
- Card
Then swap the offer structure.
Weight-loss runs on a free discovery call held by a card.
Hormone runs on a paid labs-plus-review structure.
DPC runs on a membership-first enrollment.
For hormone, the script explains the two steps plainly:
“Step one is labs — you pay the clinic three hundred dollars for a comprehensive panel. Step two is the hormone review visit, which is three hundred dollars, and if you decide to start the membership, that fee is credited toward your first month.”
For direct primary care, the framing leads with the membership:
“You enroll first, then your initial consult covers meds, refills, and your treatment plan, and ongoing access is included.”
The discovery questions also shift.
For hormone and DPC, ask:
- Whether they have a current provider
- Why they are switching
- What they are not getting now
The opening, permission-to-explain beat, assume-the-close booking, and card on file stay identical across all three paths.
That is why one script with three branches is easier to train than three separate scripts.
How do you make sure no patient-acquisition call ends without a booked next step?
Make “no call ends without a scheduled next step” the rule.
The default is always a booked appointment with a card on file.
But when a lead truly will not commit, the rep does not just hang up and lose them.
They pivot to a text:
“Totally fine. If it’s okay with you, I’ll text you our scheduling link so when you’re ready you can grab a spot before they fill up. What’s the best cell number to use?”
That captures the lead into a follow-up sequence instead of letting them evaporate.
The combination is what turns ad spend into actual booked patients:
- Same-day callback
- Discovery conversation that builds trust
- Price objection that ends in a scheduling question
- Card-on-file booking
- Never-end-without-a-next-step rule
The ads create the lead.
The phone script is where the patient acquisition actually happens.