Also Organic Social Media for Cash-Pay Medical Practices — Why It’s the Slowest Lead Source, the Highest Quality, and the Reason Everything Else Converts Better
Organic social media is the slowest lead source any cash-pay medical practice will ever run — and the highest-quality. After running every major patient-acquisition channel across 40 of the fastest-growing cash-pay clinics in the country, the pattern is consistent: organic social takes the longest to produce leads, is the most personality-driven, and books patients who are ready to schedule right now. It is also the single biggest multiplier on every other channel you run. This FAQ walks through when to start, what content actually books patients, how to monetize without a complicated funnel, and the owner-dependency downside nobody wants to talk about.
Why is organic social media the slowest lead source for a cash-pay medical practice — and also the highest quality?
Organic social takes the longest to produce leads because it builds trust one short video at a time — and that’s exactly why the leads it produces are the highest quality you’ll ever generate.
Paid ads can produce a booked patient on day one. Organic social usually cannot.
You’re:
- Publishing
- Getting watched
- Getting saved
- Getting shared
- Getting DM’d
…and then somewhere between video 30 and video 300, a viewer who has watched you talk about hormone optimization or knee pain for months decides this is the practice.
They already know:
- Your face
- Your voice
- Your offer
- How you think
They are not shopping.
Also, they are looking to book with you now.
That is the trade-off.
Organic social is:
- Very personality-driven
- Slow-compounding
- High-trust
And the quality of the leads at the end of that compounding is higher than anything a cold ad can produce.
Leads are leads — patient acquisition is patient acquisition — but the patient who walks in from a short-form video they watched for six months shows up ready to swipe a card.
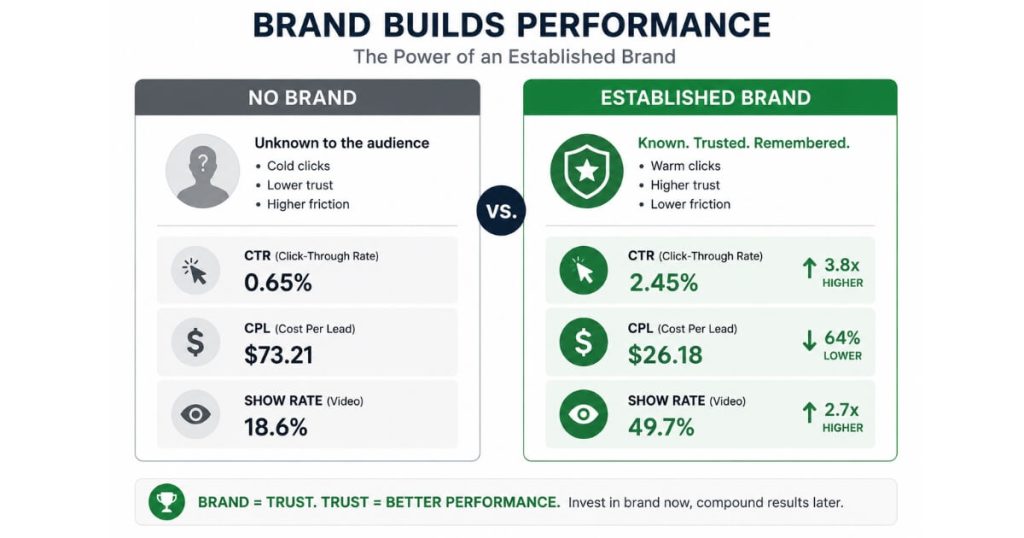
Why does an established organic brand make Facebook, TikTok, and Google ads convert dramatically better?
The better your brand is on social platforms, the better everything else converts. That’s the rule.
I wouldn’t run Facebook, Instagram, or TikTok ads unless I had an established brand first.
The reason is mechanical:
When a prospect sees a cold ad and the next thing they do is look you up — and they will look you up — what they find determines whether they book.
If your handle is a ghost town, the ad has to do all the work.
If your handle is full of:
- Patient stories
- Real procedures
- A doctor they recognize
…the ad converts at multiples of what it would have.
Same:
- Ad
- Offer
- Landing page
Different conversion rate because the brand did the lifting.
Across the 40 cash-pay clinics in our experience pool, the clinics that had established brands had everything else work really well for them.
If you’ve ever wondered why organic social makes everything convert better, it’s because trust gets built before the prospect ever lands on your website, booking page, or sales conversation. When patients already recognize the provider, understand the offer, and have consumed educational content for weeks or months, every other marketing channel starts with a smaller trust gap and a higher likelihood of conversion.
Paid social got cheaper.
Google ads converted better.
Even SEO traffic closed at a higher rate because visitors arrived already half-sold from the social presence they found while shopping around.
The brand isn’t a vanity asset — it’s the conversion multiplier sitting upstream of every channel.
One clear example:
A regenerative-medicine and aesthetics practice we worked with became the #1 stem cell expert on YouTube, hired four more doctors, and removed the owner from day-to-day operations entirely on the back of the organic brand they built.
Every other channel they run today rides on top of that brand equity.
How much does organic short-form video content actually cost to produce at scale?
A basic short-form video editor runs $100 to $150 per short, and the good ones are not cheap — which is exactly why production cost is the high barrier to scale on this channel.
The math gets uncomfortable fast.
If you want to publish one short a day across:
- TikTok
- Instagram Reels
- YouTube Shorts
…you’re staring at $3,000 to $4,500 a month in editing alone before you’ve paid for:
- Filming
- Scripting
- Thumbnails
Step up to a strong editor who actually knows:
- Pacing
- Captions
- Hook structure for medical content
…and that number climbs.
Step up to a small team that produces consistent volume and you’re now running a content department.
That’s the part most clinic owners don’t see going in.
The filming part is free if the owner does it.
The scaling part — turning raw footage into 30 polished, captioned, hook-led shorts a month, every month — is where the cost lives.
It’s why most practices either:
- Stay tiny on organic
- Or end up paying for the production capacity they need to compound
What kind of organic social content actually books cash-pay medical patients?
Story-based content books patients. “Content for content’s sake” does not.
I don’t like just making content to make content.
The clinics that win on organic social:
- Tell stories
- Are relatable
- Are empathetic
- Really understand their customer
I’m a big fan of doing cool stuff with your customers and then telling a story about it:
- A patient milestone
- A transformation
- A moment in the room
- Something you actually learned from a case
That’s the content people stop scrolling for, and it’s the content that converts a viewer into a booked discovery call.
Tactically:
- Lead with the patient’s problem in the first three seconds
- Show the moment that mattered
- Explain what you did and why in plain language
- Close on the outcome or the lesson
The hook is the story’s promise.
The body is the proof.
The end is the takeaway a viewer will share or save.
What does not work:
- Trend chases that have nothing to do with your services
- Dance overlays on serious medical content
- Generic “5 tips” videos with no patient at the center
- Content produced because a calendar said it was time to post
Cash-pay medical patients are buying a person and a practice, not a content schedule.
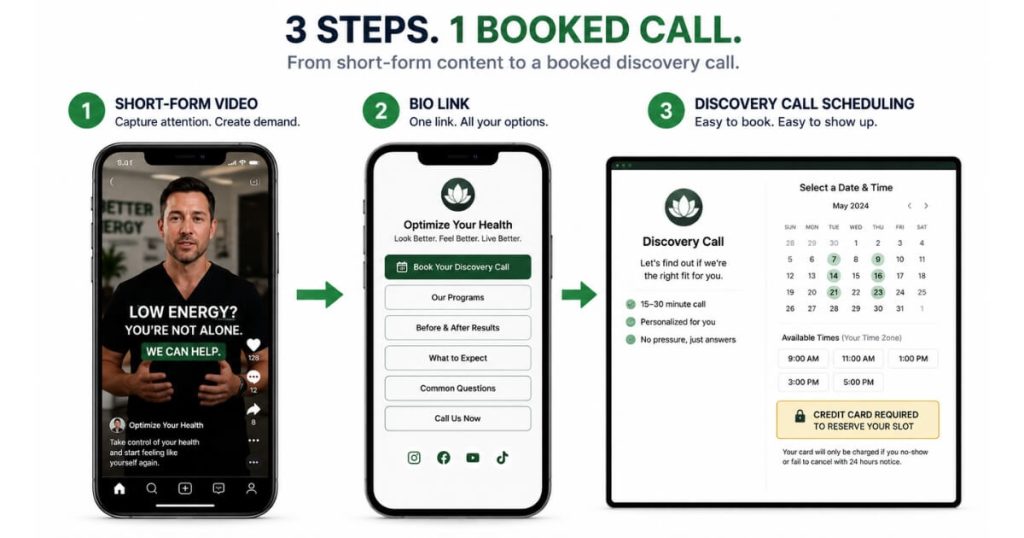
How does an owner-operator monetize organic social traffic without building a complicated funnel?
Send viewers to a free discovery call page where they put a credit card in to reserve the slot — that’s it. No complicated funnel required.
The viewer is already most-aware by the time they click your bio link.
They’ve watched you for:
- Weeks
- Months
They don’t need:
- A VSL
- A quiz
- A lead magnet
- A seven-email sequence
…to warm up.
They need a calendar with a credible commitment device on it.
The credit-card-to-reserve mechanism does the filtering work that a multi-step funnel would otherwise have to do.
They don’t pay for the appointment.
They’re just reserving the slot.
Tire-kickers don’t put in a card.
Patients who actually want to book do.
This is the single biggest win of an organic-first strategy:
Monetization is a one-page operation.
- Bio link
- Discovery call scheduling page
- Credit-card hold
- Kept appointment
That’s the whole machine.
The trust was built upstream on the video feed, so the funnel doesn’t have to manufacture it.
When should a cash-pay medical practice’s owner film their own organic content vs. hire it out?
The owner should film it themselves. I do it myself — and that’s the answer for almost every cash-pay practice.
Organic social is very personality-driven.
The face on the camera is the asset.
An agency or a hired creator can:
- Edit
- Schedule
- Repurpose
- Run the back end
But the on-camera person should be:
- The doctor
- The practitioner
- The owner the patient is going to see in the room
That’s what makes the leads pre-sold when they show up.
Outsource:
- Editing
- Captioning
- Publishing cadence
- Thumbnail design
- Comment triage
Keep the filming on the owner.
Where it can be hired out:
Practices with multiple high-personality providers can rotate on-camera duty across the team, which both spreads the load and starts to de-risk the owner-dependency problem (see the next question).
Practices with an owner who genuinely refuses to be on camera should probably pick a different primary channel:
- Paid ads
- SEO
- Events
…rather than try to fake a personality-driven channel without a personality.
What’s the downside of an owner-dependent organic brand for a cash-pay medical practice?
The downside is exactly what it sounds like:
A business dependent on the owner’s face has an owner-shaped vulnerability — if the owner stops filming, slows down, or wants to step back, lead flow on that channel stops with them.
For an owner who loves being on camera and plans to stay in the practice for the long haul, that’s not a real problem — it’s just the cost of the highest-quality lead source available.
For an owner planning to:
- Exit
- Sell
- Remove themselves from day-to-day
…an organic brand built entirely on their personal face is an asset that doesn’t fully transfer.
The clinic’s enterprise value gets tied to:
- A person
- Not a system
The fix is intentional from day one:
- Build the brand under the practice’s name as much as the owner’s
- Bring associate doctors and team members into the on-camera rotation early
- Use the organic channel’s compounding to fund the paid, SEO, and event channels that aren’t owner-dependent
Done right, the owner-led organic brand becomes the launchpad.
It produces the trust and the cash flow that lets every other channel scale, and then the practice stops being dependent on any single feed.
What’s the next step?
If you’re a cash-pay medical practice owner trying to decide whether organic social is worth the slow build — or how to use it as the brand multiplier that makes your paid ads, SEO, and events all convert better — we can map it to your specific vertical, your offer, and your capacity to be on camera.
We’ve done this across 40 of the fastest-growing cash-pay clinics in the country, and the pattern is repeatable when the channel order is right.