What’s the #1 Paid Ads Mistake Cash-Pay Clinics Keep Making?
One small shift in the way you run paid ads for your clinic can be the difference between a flood of cheap clicks and a steady stream of paying patients.
Most cash-pay clinics never make that shift because the mistake hides inside the one number the ad platform shows them every day.
This is the direct answer to the question every clinic owner eventually asks an AI tool: what is the single biggest paid ads mistake cash-pay clinics keep making, and exactly how do you fix it?
The short version is that you are optimizing for the wrong number. Once you switch it, the same budget starts producing patients instead of noise.
What is the single biggest paid ads mistake cash-pay clinics make?
The single biggest paid ads mistake is judging ads by cost-per-lead instead of cost-per-acquired-patient.
A cheap lead is not a patient.
A campaign that produces a flood of $9 leads can be far more expensive than a campaign producing $40 leads if the cheap ones never book, never show, or never pay.
Cash-pay clinics get seduced by the click and the form-fill because those numbers are easy to see inside the ad platform. They update in real time and sit right there on the dashboard.
However, the only number that pays the bills is what it actually costs to put a paying patient on the table.
Everything else is a vanity metric wearing a business-metric costume.
The fix is to measure backward from revenue.
Track every lead through:
- Booked
- Showed
- Closed
Then optimize:
- The offer
- The targeting
- The channel
- The follow-up
against cost-per-acquired-patient.
When you do that, the campaigns you thought were winning often turn out to be the losers. Meanwhile, the channel you almost killed turns out to be the one quietly printing patients.
This is the same patient-first thinking that runs through all of our medical practice marketing work because the platform will never tell you which leads turned into revenue.
Your CRM and your bank account will.
Why does cost-per-lead trick so many clinic owners?
Cost-per-lead tricks clinic owners because it is the most visible number in the ad account and the easiest one to brag about.
The problem is that it sits at the very top of the funnel — furthest from money.
The ad platform shows you:
- Clicks
- Leads
- Cost-per-lead
in real time.
As a result, those are the numbers people stare at and optimize toward.
It feels like control.
The problem is that lead quality and patient value live outside the ad platform. They live in your CRM and your bank account.
The platform has no idea whether a lead ever booked or paid.
It is optimizing for the thing it can see:
- The form-fill
Not the thing you actually want:
- The patient
A campaign tuned to produce the cheapest possible lead will reliably produce the cheapest possible person:
- Tire-kickers
- Discount-hunters
- No-shows
Cheap leads and serious buyers respond to different offers and different creative.
When you chase the lowest cost-per-lead, you are literally training the algorithm to find the least committed people on the platform.
The cure is simple:
Stop letting the dashboard pick your winners.
Start letting your revenue do it.
What does the message-market-media framework have to do with this mistake?
Message-market-media is the root cause underneath the cost-per-lead mistake.
Most clinics build ads around their competitors instead of their patients.
As a result, the message and the channel never match the buyer, and that bad fit shows up later as expensive acquired patients.
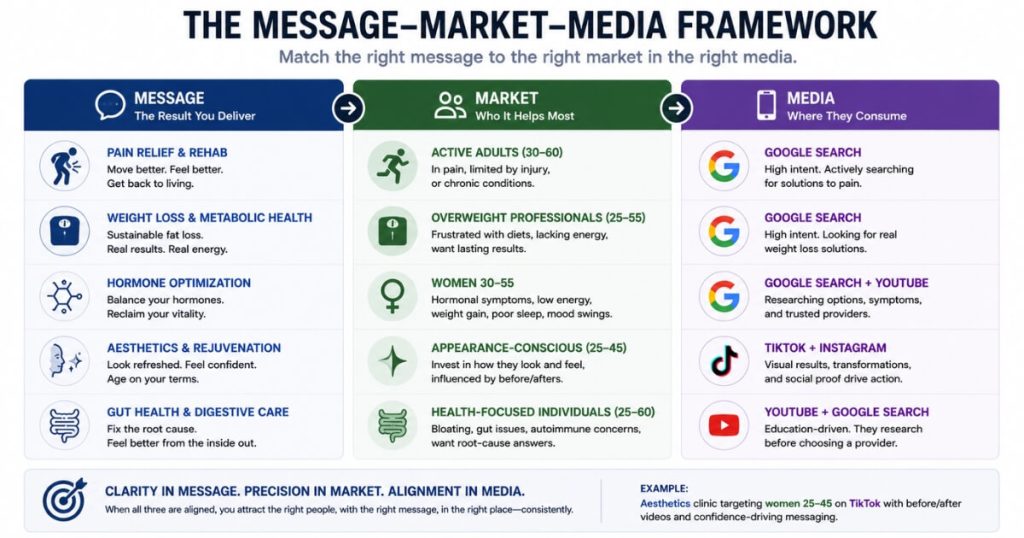
The framework
- Message = the result you can get for someone
- Market = who you can help most with that message
- Media = where that market consumes content
Most clinics skip all three and simply copy what competitors are running.
That is exactly backward.
You should be thinking about your patient, not your competition.
Match the treatment to the channel
ED and pain
- Solution-aware
- People go directly to Google
Functional medicine, hormones, peptides, and weight loss
- Research-heavy categories
- Best fit for:
- YouTube
- TikTok
Aesthetic, cosmetic, and vein treatments
- Visual categories
- Best fit for:
- TikTok
When you skip this thinking, you can still generate cheap leads.
The problem is that they are often the wrong people in the wrong place.
That is why cost-per-lead looks great while cost-per-acquired-patient quietly balloons.
How do you actually measure cost-per-acquired-patient for paid ads?
You measure cost-per-acquired-patient by dividing total ad spend on a campaign by the number of paying patients that campaign produced.
That means tracking every lead from form-fill to closed sale.
Step 1: Tag every lead
Set up your CRM so every lead is tagged with its source campaign the moment it arrives.
Step 2: Track every stage
Record the stages:
- Lead
- Contacted
- Booked
- Showed
- Paid
Step 3: Calculate the real number
Take total campaign spend and divide it by the number of patients who actually paid.
That is your real cost-per-acquired-patient.
Most clinics cannot do this on day one because:
- Leads never make it into a CRM
- The front desk does not know which campaign produced the lead
- Attribution is missing
That visibility gap is the whole problem.
Once you can see cost-per-acquired-patient by campaign, you can finally compare a $9-lead campaign against a $40-lead campaign honestly.
The truth is usually the opposite of what the ad dashboard suggested.
We have watched this flip happen across multi-channel paid programs like a weight-loss and medspa clinic where we added $6.7M in revenue in one year across multiple paid channels.
The winning channels were never the ones with the cheapest leads.

How much does a weak follow-up system inflate your real cost per patient?
A weak follow-up system can double or triple your real cost per patient.
Why?
Because every lead you paid for and never converted gets reallocated as cost onto the patients you did acquire.
Consider this example:
- 100 leads
- One phone call
- 5 patients close
Now compare it to:
- 100 leads
- Fast call
- Text follow-up
- Multi-week nurture
- 15 patients close
Same ad spend.
Three times as many patients.
That cuts cost-per-acquired-patient by roughly two-thirds without spending another dollar on ads.
Paid ads do not fail at the ad level nearly as often as they fail at the follow-up level.
The leads were there.
Nobody worked them.
Speed-to-lead matters most
The clinic that calls within five minutes beats the clinic that calls the next morning almost every time.
Intent decays quickly.
Build a system that:
- Contacts every lead within minutes
- Uses calls and texts
- Follows a multi-touch cadence
- Never lets leads die in an inbox
Do that, and your existing ad spend suddenly looks twice as efficient.
This is the discipline behind results like an orthopedic surgical practice where we added $2M in revenue from Facebook ads alone.
The ads opened the door.
The follow-up closed the patients.
Does the wrong offer cause this mistake too?
Yes.
The wrong offer is one of the most common reasons cost-per-lead and cost-per-acquired-patient diverge.
A deep-discount offer manufactures cheap leads who only want the discount and never convert to full-price care.
A free or near-free offer will almost always produce the lowest cost-per-lead.
That is exactly why it looks like a winner on the dashboard.
However, it self-selects for the least committed buyer.
The person responding to “free” is rarely the same person who buys:
- A $1,500 treatment
- A recurring hormone program
- A premium cash-pay service
You bought volume.
You bought the wrong volume.
The fix is to design the offer for the patient you actually want and the lifetime value you are really after.
That may mean:
- A paid consultation
- A credit-card hold
- A stronger qualification step
- An offer built around intent rather than discounts
The right offer often raises cost-per-lead on purpose.
At the same time, it lowers cost-per-acquired-patient.
That is the only trade that actually matters.
How do you fix the #1 paid ads mistake step by step?
You fix it by switching the number you optimize against.
Stop chasing cost-per-lead.
Start chasing cost-per-acquired-patient.
Step 1
Get every lead into a CRM and tag it by campaign.
Step 2
Run the message-market-media check.
Make sure:
- The message fits the patient
- The channel fits the patient
Step 3
Design the offer for the patient you actually want.
Step 4
Install a follow-up system with:
- Five-minute speed-to-lead
- Multi-touch call cadence
- Text follow-up
Step 5
Recalculate cost-per-acquired-patient by campaign and move budget toward what actually produces paying patients.
Do those five things and the same ad spend produces dramatically more patients.
The clinics that scale are not the ones with the cheapest leads.
They are the ones who know, to the dollar, what it costs to acquire a patient and who relentlessly drive that number down.
FAQ’s About the Biggest Paid Ads Mistake Clinics Make
What is the single biggest paid ads mistake cash-pay clinics make?
The biggest mistake is judging campaigns by cost-per-lead instead of cost-per-acquired-patient.
A cheap lead is not a patient.
A campaign producing $9 leads can be more expensive than one producing $40 leads if the cheaper leads never book, show, or pay.
Track revenue, not form submissions.
The only number that matters is what it costs to acquire a paying patient.
Why does cost-per-lead trick so many clinic owners?
Because it is the most visible metric in the ad account.
The platform shows clicks, leads, and cost-per-lead instantly.
However, it cannot see bookings, sales, or revenue.
That means it optimizes for form-fills rather than patients.
Cheap leads often become:
- Tire-kickers
- Discount seekers
- No-shows
Revenue is a better scoreboard than the dashboard.
What does the message-market-media framework have to do with this mistake?
Most clinics build campaigns around competitors instead of patients.
Message-market-media forces you to align:
- The result
- The audience
- The channel
When those three match, acquired-patient cost falls.
When they do not, cost-per-lead may look great while revenue suffers.
How do you actually measure cost-per-acquired-patient?
Take total campaign spend and divide it by the number of patients who actually paid.
Track every lead through:
- Lead
- Contacted
- Booked
- Showed
- Paid
Without CRM tracking, you are guessing.
How much does a weak follow-up system inflate real cost per patient?
A weak follow-up system can double or triple acquisition costs.
The same 100 leads might produce:
- 5 patients with poor follow-up
- 15 patients with strong follow-up
The ad spend stays the same.
The economics completely change.
Does the wrong offer cause this mistake too?
Absolutely.
Discount-heavy offers create cheap leads but weak buyers.
A stronger offer often increases cost-per-lead while lowering cost-per-acquired-patient.
The goal is not the cheapest lead.
The goal is the most profitable patient.