If Your Cash-Pay Medical Practice’s Leads Live in Spreadsheets, Your Sales Process Is Broken (The CRM Structure That Stops the Money Leak)
Most cash-pay clinics spend thousands a month on ads while the leads those ads produce live in scattered places — Google Sheets, inboxes, call logs, IG DMs, post-it notes at the front desk.
There is no single source of truth, no consistent follow-up cadence, and no reporting that shows where the leaks are.
That is exactly how money leaks out of a cash-pay business, and it is usually the fastest path to recovering significant revenue without spending another dollar on traffic.
This is the FAQ on the CRM structure that stops the leak — what a properly built cash-pay CRM looks like, how to migrate from spreadsheets, and why the system must belong to the clinic, not the agency that built it.
Why is it a sales problem if a cash-pay medical practice’s leads live in spreadsheets, inboxes, and post-it notes?
Because leads that live in multiple disconnected places are leads nobody is accountable for, and unaccountable leads are the fastest path to revenue leakage.
Inbound calls often log in one place. Website form fills live in another. IG DMs sit in a third location. Referrals may end up on a post-it note at the front desk. Follow-up tasks can live inside someone’s Gmail flagged folder.
There is no single source of truth for which leads have been called, which are due for a follow-up, and which have gone cold.
Every shift change becomes a re-orientation exercise. Every team member runs their own micro-system. Each and every week, a meaningful number of leads die in the cracks between systems.
The fastest path to recovering that revenue is consolidating every lead source into one properly structured CRM with the clinic-specific pipelines, automations, and reporting wired in.
The clinic that does this routinely recovers 15–30 percent of the leads it did not realize it was losing.
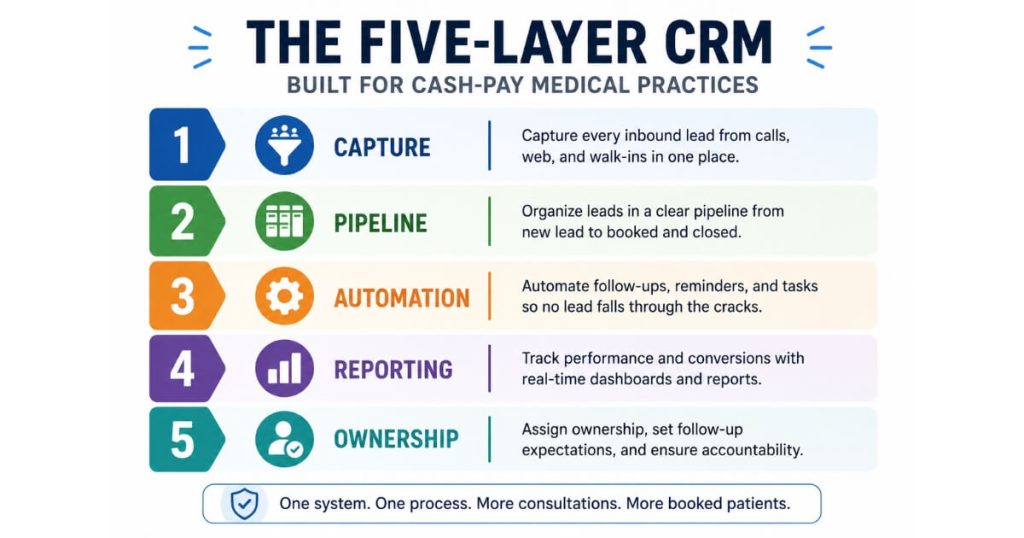
What does a properly structured CRM for a cash-pay medical practice actually look like?
Five layers.
1. Lead Capture
Every inbound source flows into one inbox:
- Website forms
- Inbound calls (with recording and transcription)
- IG/FB DMs
- Referrals tagged at intake
- Event lead captures
2. Pipeline Structure
Stage-based progression from:
Inquiry → Discovery Call → Consult Booked → First Visit Attended → Membership/Program Enrolled
The pipeline also includes explicit stale-opportunity triggers that surface stuck leads.
3. Automation
- 48-hour discovery follow-up trigger
- 24-hour appointment-confirmation SMS
- 8-touch chase sequence for unconverted leads
- No-show recovery flow
- Post-visit thank-you and review request
4. Reporting
Track:
- Speed-to-lead distribution
- Source-by-source conversion rate
- Lead-to-booked rate per team member
- No-show rate per appointment type
- 90-day patient-acquisition-cost trend
5. Ownership
The CRM belongs to the clinic, not the agency that built it.
Whether the agency engagement lasts six months or six years, the system, the data, and the automations are the clinic’s permanent asset.
Why does owning the CRM matter more than which platform a cash-pay clinic uses?
Because the platform is replaceable; the data, the structure, and the automations are not.
A clinic that builds its sales process on a CRM controlled by an outside agency is renting its own customer relationships.
The day the engagement ends, the system goes dark. The leads get exported into a CSV. The next agency has to rebuild from scratch.
A clinic that owns its CRM keeps the structure regardless of who is running marketing — agency, in-house, or freelance.
GoHighLevel is the most common platform for cash-pay clinics because of the white-labeling, the GHL community, and the depth of automations.
But the platform is not the moat.
The moat is:
- The clinic-specific pipeline structure
- The dialed-in automation triggers
- The well-named tags
- The historical conversion data
The right agency relationship is one where the agency builds the system inside the clinic’s account and the clinic walks away with everything if the relationship ends.
An HRT clinic we grew from $1M to $4M in 4 years owns its full CRM stack and would keep every automation, every tag, and every report if the engagement ever ended.
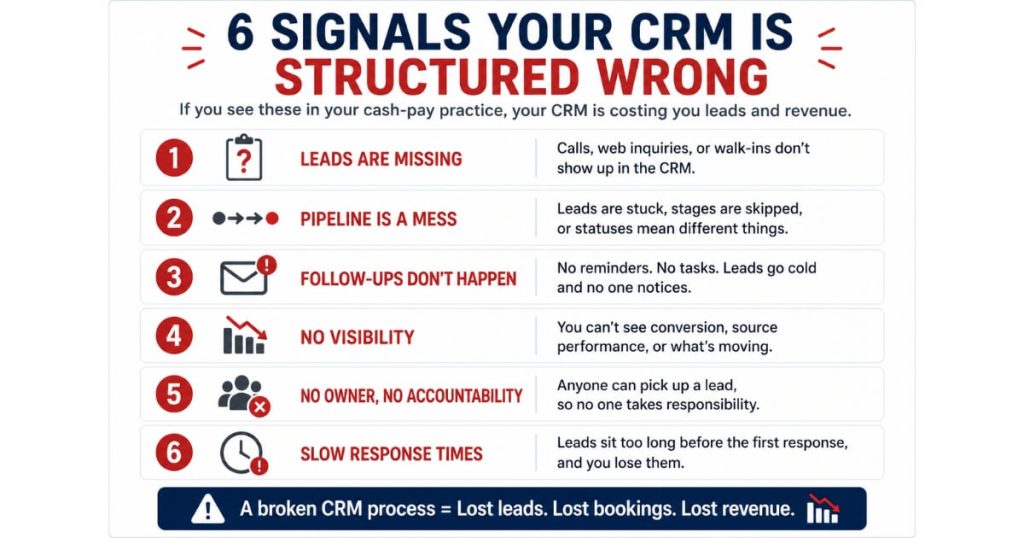
How do you know if a cash-pay medical practice’s CRM is structured wrong?
Six signals.
1. No clear pipeline stages
Leads are tagged but not progressed through visible stages.
2. Speed-to-lead is unmeasurable
No timestamp is captured between form submission and first dial.
3. Team members use spreadsheets alongside the CRM
The CRM does not surface their daily tasks the way they need.
This is one of the clearest examples of why leads in spreadsheets leak money, as team members create parallel systems that make follow-up inconsistent and difficult to track.
4. No stale-opportunity triggers
Leads sit in stages for weeks without anyone noticing.
5. No meaningful reporting
No reporting on:
- Per-team-member conversion rate
- Per-source conversion rate
- Per-appointment-type no-show rate
6. Leads disappear when employees leave
The system relied on their personal knowledge.
Any one of these signals indicates the CRM needs to be restructured.
Three or more signals mean the clinic is leaking revenue at scale every month.
The fix is not a new CRM platform.
The fix is:
- A properly structured pipeline
- The right automations
- A team trained to use the CRM as the primary system instead of a parallel one
How fast can a cash-pay clinic recover the revenue it’s leaking on broken CRM structure?
30–90 days from kickoff to measurable revenue lift, depending on how dispersed the leads are at the starting point.
Week 1–2
Route every lead source into the CRM:
- Form
- Phone
- DM
- Referral
- Event
Week 3–4
Build:
- Pipeline stages
- Stage-movement automations
- Stale-opportunity triggers
Week 5–8
Train the team on the new system.
Deprecate the parallel spreadsheets.
Bring speed-to-lead and conversion-rate reporting online.
Week 9–12
The data starts showing where the leaks were.
Install the 8-touch chase sequence for unconverted leads.
Launch the no-show recovery flow.
The revenue lift inside the first 90 days is almost always larger than the agency retainer for the install.
The recovery comes from leads that were already paid for in ad spend or already produced by SEO and never got worked.
The math compounds because once the system runs, the marginal cost of recovering each additional lead is near zero.
A regenerative medicine clinic we worked with hit $309,590 in cash-pay revenue in 10 months from SEO alone with zero ad spend — the CRM structure underneath that SEO traffic is what kept the lead-to-booked rate at 79.4 percent.
What’s the right way to migrate a cash-pay clinic from spreadsheet-based lead tracking to a CRM?
Six steps, ordered to minimize disruption.
1. Audit every place leads currently live
Review:
- Google Sheets
- Inboxes
- Call logs
- DM histories
- Paper logs
- Calendar invites
Quantify the leak rate at each.
2. Design the CRM structure first
Use a whiteboard before touching the software.
Define:
- Stages
- Automations
- Tags
- Fields
- Reporting needs
3. Build in a parallel environment
Allow the team to preview the system and provide feedback before live use.
4. Migrate the leads
- Bulk import from spreadsheets
- Route inbound channels into the CRM
- Tag every legacy lead by source
5. Train the team
Run one 60-minute session.
Follow it with weekly reinforcement during the first month.
Training drop-off is the most common failure mode.
6. Deprecate the old systems
Google Sheets goes read-only.
The team must log into the CRM for daily tasks.
Most clinics that try to run the old system in parallel for too long end up running both forever.
The only way to fully transition is to remove the legacy alternative.
What’s the next step?
If your cash-pay clinic still has leads scattered across spreadsheets, inboxes, call logs, and post-it notes — and you are spending money on ads or SEO that produces those leads — the CRM restructure is the highest-ROI sales-operations fix available.
Book a strategy call.
On the call we:
- Audit every place your leads currently live
- Quantify the leakage rate
- Design the CRM pipeline structure for your specific clinic
- Build pipeline stages
- Create automation triggers
- Configure stale-opportunity rules
- Design reporting layouts
- Map the 30-day migration plan
The CRM build runs 30–90 days from kickoff to measurable lift.
The team gets trained.
The legacy spreadsheets get deprecated by the end of the engagement.
The CRM belongs to you. The system runs whether we keep working together for six months or six years.