How Do You Keep Weight-Loss Patients From Quitting After 90 Days?
The hardest part of running a GLP-1 weight-loss program is not getting patients in the door — demand makes that easy.
The hard part is the middle.
Somewhere around the fourth order, roughly the 90-day mark, patients quietly dwindle away.
The novelty fades. They hit a number they like or stall on a plateau. And the follow-up goes silent right when they are deciding whether to keep going.
Every one of those patients was a recurring revenue stream you already paid to acquire.
This is the field playbook for keeping weight-loss patients — and the revenue — past the drop-off cliff: the milestone communications, the maintenance offer, and the journey design that turns the leaky middle of the program into the most valuable book of business you have.
Why do weight-loss patients quit around the 90-day mark?
Because three things converge at roughly the fourth order:
- The early novelty wears off.
- The patient has either hit a number they are happy with or stalled on a plateau.
- Your follow-up cadence usually goes quiet right when they are deciding whether to continue.
In practice, the drop-off is not at the first order.
It is around four months in.
Patients order, reorder, and then start to dwindle after that fourth pickup.
The front end feels like the hard part, so that is where clinics put their energy:
- The offer
- The consult
- The first set of four pre-filled syringes
But getting a GLP-1 patient started is the easy part because demand is high.
The unglamorous middle — visit two, three, four — is where the leak happens.
There is no automated journey.
The personalized texts get inconsistent.
And the patient quietly decides the program is optional.
There is also a knowledge gap working against you.
Patients who reach their goal believe stopping is the successful ending.
They do not know that quitting cold turkey makes them more likely to regain the weight.
So they exit on a high note.
Then you do not hear from them again until the weight is back.
Retention starts with accepting that the 90-day cliff is structural, not random.
Most of the moving parts here live inside the same playbook we use for med spa marketing, where recurring weight-loss revenue is won or lost in the follow-up.
What does a retention journey for GLP-1 patients actually look like?
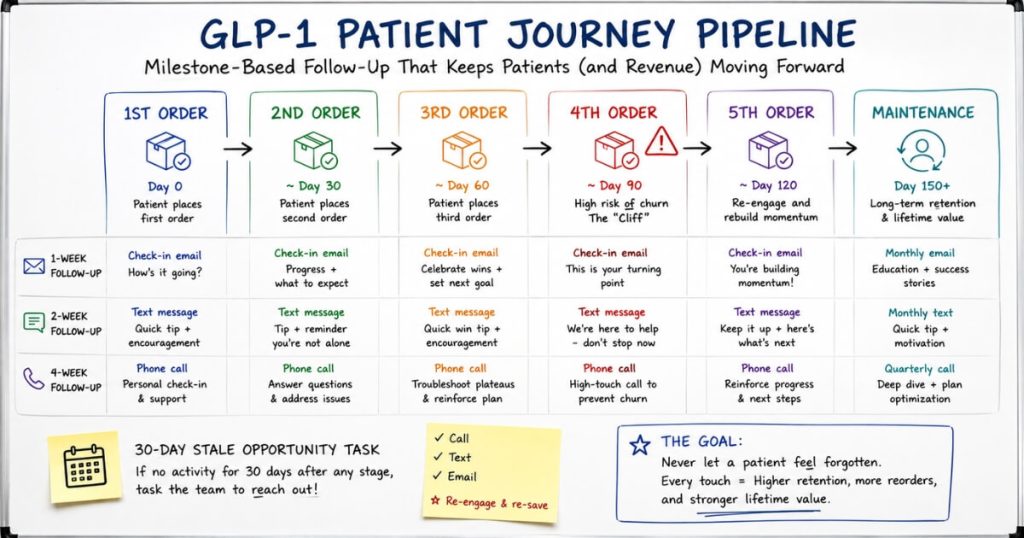
It is a milestone-based pipeline keyed to orders, not dates.
That means it includes a check-in at one week, two weeks, and four weeks.
It also includes an automatic follow-up task whenever a patient goes stale.
The structure we build for weight-loss clinics is a pipeline with a stage for every order:
- First order
- Second order
- Third order
- Fourth order
- Maintenance
Patients move forward only when they actually complete an order.
They do not move forward just because a calendar timer fires.
Date-based automation lies to you about where a patient really is.
Order-based stages reflect reality.
When someone comes in for their third pickup, they go into the third-order-completed column.
Then the system knows precisely who is due for what.
The cadence inside the journey is deliberately light.
New patients get a short four-to-five-day check-in:
“How did your first injection feel?”
Then they get a two-week touch.
Then they get a four-week touch only if the patient has not already rebooked.
Much of the time, by the time you work through the four-week list, people are already back on the schedule.
The single most important mechanic is the stale-opportunity rule.
If a patient sits in any stage for 30 days without progressing, the system automatically creates a task to follow up.
That one rule stops patients from silently falling through the cracks between orders.
That is where almost all preventable churn actually happens.
The journey is a hybrid by design.
Automation moves people between stages and surfaces the tasks.
But a human confirms each patient is genuinely scheduled.
As one operator put it, water finds the cracks.
The system works only if someone actually checks their tasks.
How do milestone check-ins reduce churn without annoying patients?
By replacing a high volume of generic blasts with a few well-timed, personalized touches tied to where the patient actually is in their program.
The annoyance risk is real.
When a clinic adds a monthly newsletter on top of an existing two-week and four-week text cadence, some patients will ask to be removed from the email list even though they are still active.
That is not a sign that follow-up is bad.
It is a sign the cadence got too dense.
The fix is to consolidate, not pile on.
Keep a one-week new-patient check.
Then meet in the middle with a single three-week touch instead of separate two- and four-week messages.
Fewer, better-timed touches feel like support.
A steady drip of generic messages feels like pestering.
Tone is the other half of the equation.
Every touch should read as service, not sales.
At each visit, tell the patient explicitly to call or text with any questions.
That way, when a proactive message arrives, it lands as:
“We are on top of your care.”
Not:
“We abandoned you for a month and now we want money.”
A check-in seven days before a patient runs out should read like a favor:
“Our records show you are due for a refill, and we wanted to help you get priority scheduling for your next visit.”
Personalized messaging that looks like a human wrote it outperforms an obvious mass blast every time.
A patient who feels known is a patient who keeps coming back.
Should I put weight-loss patients on a membership or auto-bill to stop churn?
A membership helps.
But a blind auto-bill that charges the card without shipping medication backfires.
So does a system that leaves refills entirely in the patient’s hands.
The journey design matters more than the billing mechanic.
The tempting shortcut is to solve for predictable revenue with a subscription that runs the card every 30 days.
The problem is that many patients stretch four weeks of medication into five or six.
So the billing date and the actual reorder date drift apart fast.
If you bill and do not deliver, patients are rightly furious.
If you ship everything up front and rely on them to reorder, you have handed them too much control.
You have also erased the touchpoint that drives retention.
Either extreme breaks the relationship.
A membership works when it is built correctly.
That means it is paired with a clear membership agreement the patient signs acknowledging the recurring charge.
It also has to be structured so the discount is genuinely worth it.
A small monthly fee for fifty percent off only pencils out for higher-dose patients.
So membership is a lever for a segment of your book — not a universal cure.
The durable answer is the journey itself:
- Keep the recurring visit.
- Keep the human follow-up.
- Let membership reinforce the relationship rather than replace it.
Eternity Health Partners, a membership practice that retains roughly 250 members, holds those patients because the relationship is built on visits and education, not just a card on file.
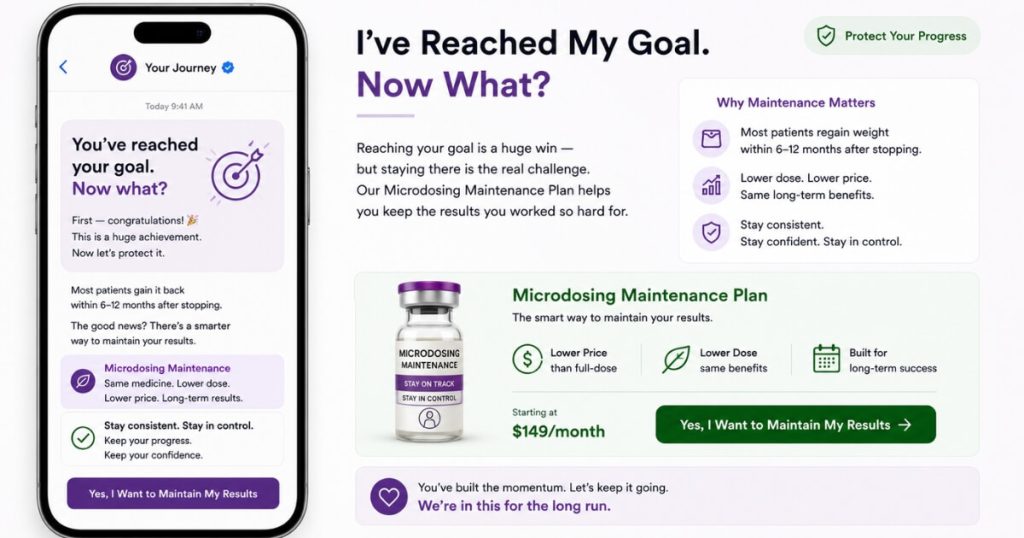
How do you keep patients who reach their goal weight from leaving?
You build a maintenance offer and a reframe that turns “I’m done” into “now what?” before the patient has mentally exited the program.
Goal-reachers are the highest-risk churn group precisely because, to them, success means stopping.
The clinics that retain them get ahead of the moment with education.
A newsletter or milestone message built around “I’ve reached my goal — now what?” reframes the finish line as a transition.
It introduces microdosing as the next phase.
It also explains why quitting cold turkey makes weight regain more likely.
You are not selling a refill.
You are protecting the result the patient worked for.
The offer has to match the message, or the reframe collapses.
If your starting dose and your microdose cost the same, you are effectively charging patients full price to taper down.
That quietly pushes them to quit.
A dedicated, lower microdosing price point removes that penalty.
It makes maintenance the obvious choice.
Small price differences feel minor on a single patient.
But across a whole panel of goal-reachers, they add up to a materially larger retained book.
Operationally, treat the fourth-order-completed stage as your upsell and reactivation list.
These patients have proven they value the outcome.
So this is exactly where you find opportunities to retain them into:
- Maintenance dosing
- Hormone or wellness services
- Whatever your service ladder offers next
Some patients simply settle into a permanent maintenance dose and stay for years.
That maintenance segment is the most valuable book of business a weight-loss clinic can build.
This compounding-retention dynamic is what powered NuLevel Wellness Medspa to $6.7M per year on the back of GLP-1 and weight-loss patients.
Acquisition opened the door.
Retention scaled the revenue.
How do you win back GLP-1 patients who have already lapsed?
You keep lapsed patients in a defined reactivation track and check in deliberately weeks or months after they go quiet.
A surprising share come back on their own terms once the weight starts returning.
The worst move is deleting a patient from the follow-up list the instant they miss a reorder.
Unless a patient explicitly tells you they have discontinued care, they should move into a use-your-best-judgment reactivation column.
Not off the board.
Plenty of patients go quiet for reasons that have nothing to do with quitting:
- They were traveling.
- Life got busy.
- They never texted back.
Those people are not lost.
They are dormant.
The reactivation play is patient and low-pressure.
Wait anywhere from two weeks to a month or two after a patient goes stale.
Then check in.
A meaningful number book again.
And the line clinics hear repeatedly is some version of:
“I was going to stop the medication, but I’m gaining the weight back — can I reschedule?”
That reframe sells itself.
Your only job is to still be in contact when it happens.
The stale-opportunity task every 30 days keeps lapsed patients visible.
A periodic, well-timed touch tied to the very real regain risk converts a real percentage of them back into active, paying patients.
And it does that at a fraction of what it costs to acquire a new one.
FAQ’s About Weight-Loss Patient Retention
Why do weight-loss patients quit around the 90-day mark?
Because three things converge at roughly the fourth order:
- The early novelty wears off.
- The patient has either hit a number they are happy with or stalled on a plateau.
- Your follow-up cadence usually goes quiet right when they are deciding whether to continue.
In practice, the drop-off shows up around the four-month mark.
Patients dwindle away after that fourth order, not the first.
The mistake clinics make is treating the front end as the hard part.
Getting a GLP-1 patient in the door and on their first four pre-filled syringes is the easy part because demand is high and the offer is obvious.
The hard part is the unglamorous middle — visit two, three, four.
That is where there is no automated journey, the personalized texts get inconsistent, and the patient quietly decides the program is optional.
Patients who have hit their goal also genuinely do not know that quitting cold turkey makes them more likely to regain the weight.
So in their mind, stopping is a reasonable, successful exit rather than the start of a rebound.
If nobody reframes that for them at the right milestone, they leave on a high note and never come back until the weight is already back.
What does a retention journey for GLP-1 patients actually look like?
It is a milestone-based pipeline keyed to orders, not dates.
The journey we build for weight-loss clinics has a stage for every order:
- First order
- Second order
- Third order
- Fourth order
- Maintenance
Patients move forward only when they actually complete an order.
They do not move forward just because a calendar timer fires.
New patients get a short four-to-five-day check-in:
“How did your first injection feel?”
Then they get a two-week touch.
Then they get a four-week touch only if they have not already rebooked.
The personalized feel matters.
Patients respond to messages that read like a human wrote them.
So the cadence is a hybrid.
Automation moves people between stages and surfaces tasks.
But a staff member confirms each one is actually scheduled.
The single most important piece is the stale-opportunity rule.
If a patient sits in any stage for 30 days without progressing, the system creates a task to follow up.
That one mechanic stops patients from silently falling through the cracks between orders.
And that is where almost all preventable churn happens.
How do milestone check-ins reduce churn without annoying patients?
By replacing a high volume of generic blasts with a few well-timed, personalized touches tied to where the patient actually is in their program.
The risk is real.
When a clinic layers a new monthly newsletter on top of an existing two-week and four-week text cadence, some patients will ask to be removed from the list even though they are still active.
That is the signal that the cadence is too dense.
Not that follow-up is bad.
The fix is to consolidate rather than pile on:
- One-week new-patient check
- One three-week touch instead of separate two- and four-week messages
That way, patients feel supported rather than pestered.
Frame every touch as service, not sales.
At each visit, tell the patient to call or text with any questions.
Then the proactive message lands as:
“We are on top of your care.”
Not:
“Buy more.”
A good check-in seven days before they run out reads like priority scheduling:
“Our records show you are due for a refill, and we wanted to help you get your next visit on the books first.”
That tone is the difference between a touch that retains and a touch that gets you unsubscribed.
Should I put weight-loss patients on a membership or auto-bill to stop churn?
A membership helps.
But a blind auto-bill that charges the card without shipping medication backfires.
So does a system that leaves refills entirely in the patient’s hands.
The journey design matters more than the billing mechanic.
The trap is solving for predictable revenue by setting up a subscription that runs the card every 30 days.
But the patient may be stretching four weeks of medication into five or six.
If you bill and do not deliver, patients are rightly angry.
If you ship everything up front and rely on them to reorder, you have put too much in their hands and lost the touchpoint that drives retention.
A membership works when it is paired with a clear membership agreement that the patient signs acknowledging the recurring charge.
It also works when the discount is meaningful enough to be worth it.
A small monthly fee for fifty percent off only pencils out for higher-dose patients.
So it is not a universal fix.
The durable answer is the journey:
- Keep the recurring visit.
- Keep the human follow-up.
- Use membership as one retention lever rather than the whole strategy.
Eternity Health Partners, a membership practice we work with, retains roughly 250 members precisely because the recurring relationship is built on visits and education, not just a card on file.
How do you keep patients who reach their goal weight from leaving?
You build a maintenance offer and a reframe that turns “I’m done” into “now what?” before the patient has mentally exited the program.
Patients who hit their goal are the highest-risk churn group because, to them, success means stopping.
The clinics that retain them get ahead of it with education.
A newsletter or milestone message built around “I’ve reached my goal — now what?” explains microdosing as the next phase.
It also spells out why quitting cold turkey makes weight regain more likely.
The offer has to match the message.
If your starting dose and your microdose cost the same, you are quietly punishing the patient for tapering down.
So a dedicated lower microdosing price point removes the financial reason to quit.
It makes maintenance the obvious path.
Treat the fourth-order-completed stage as your upsell and reactivation list.
These are the patients who have proven they value the outcome.
So it is also where you find opportunities to retain them for other services.
Some patients simply settle into a permanent maintenance dose and stay for years.
That maintenance segment is the most valuable book of business a weight-loss clinic can build.
How do you win back GLP-1 patients who have already lapsed?
You keep lapsed patients in a defined reactivation track and check in deliberately weeks or months after they go quiet.
A surprising share come back on their own terms once the weight starts returning.
The worst thing a clinic can do is delete a patient from the follow-up list the moment they miss a reorder.
Unless a patient explicitly says they have discontinued care, they should move into a use-your-best-judgment reactivation column rather than off the board.
If a patient went stale because they were traveling, busy, or just never replied, a gentle check-in two weeks to a month or two later books a meaningful number of them.
The line clinics hear over and over is:
“I was going to stop, but I’m gaining the weight back. Can I reschedule?”
That reframe sells itself.
You just have to still be in contact when it happens.
The discipline is simply not abandoning people.
A stale-opportunity task every 30 days keeps lapsed patients visible.
A periodic, low-pressure touch tied to the regain risk converts a real percentage of them back into active, paying patients.