How Should a Cash-Pay Medical Practice Pick a Marketing Agency? (The 7 Questions to Ask Before You Hire)
Most cash-pay clinic owners pick a marketing agency the wrong way. They look at the agency’s website, ask for a few sample ads, and sign a retainer. Twelve months later the retainer has spent $60K, the lead volume looks fine in screenshots, and the clinic’s actual revenue has barely moved. This is the FAQ on how to interview a marketing agency for a cash-pay medical practice — and the seven specific questions that separate an agency that will compound the clinic’s revenue from one that will compound the agency’s retainer.
How should a cash-pay medical practice owner pick a marketing agency?
Ask seven questions before hiring any agency
1. Does the agency have at least three named, public case studies in your specific vertical (HRT, regenerative medicine, functional medicine, GLP-1, longevity, aesthetic) and can they show before-and-after revenue numbers, not just lead counts?
2. Who actually does the work day to day, what is their experience level, and how many other clinics are they running in parallel?
3. What does the operational handoff between marketing and clinic look like (CRM, lead routing, front desk training), because marketing that does not connect to the front desk leaks half the spend?
4. What is the retainer math, and what cash-pay revenue does that retainer need to produce for the relationship to be positive ROI inside 90 days?
5. What is the termination clause, and can the clinic exit cleanly if the agency is not producing?
6. What proof does the agency have that their playbook works without paid ads, because the most profitable cash-pay clinics ultimately scale on owned audience, not rented?
7. Will the agency talk to two of their current clients before you sign, so you can verify the experience matches the pitch?
Any agency that refuses the seventh question is the wrong agency.
What’s the difference between a generic marketing agency and one that specializes in cash-pay medical practices?
A generic agency optimizes:
- lead volume
- cost per lead
A cash-pay specialist optimizes:
- front-desk-to-booked-patient conversion rate
- membership LTV
- recurring revenue ratio
Because in cash-pay medicine those are the only numbers that matter.
Why lead volume is rarely the bottleneck
Lead volume is upstream of revenue, but the leads are typically not the bottleneck at a cash-pay clinic doing $1M+.
The bottleneck is:
- the front desk
- the offer structure
- the pricing of the first visit
- the retention engine
A generic agency cannot fix any of those.
They will pour more leads into a leaky front desk and call the resulting CPL spike “platform inflation.”
A cash-pay specialist will:
- pause the ad spend
- fix the conversion rate
- install or restructure the membership model
- turn the ad spend back on at a higher unit profitability
The proof that an agency actually specializes in cash-pay medicine
The proof that an agency is actually a cash-pay specialist is named clients in cash-pay verticals with public case studies showing membership growth and recurring revenue — not just lead counts.
An HRT clinic we grew from $1M to $4M in 4 years hit those numbers because the work was as much front-desk and membership operations as it was advertising.

What red flags should I watch for when interviewing a marketing agency for my cash-pay medical practice?
Five red flags
- The agency cannot name three clients in your specific vertical.
- The proof they show is impressions, reach, or click-through rate rather than revenue, booked patients, or membership growth.
- The discovery call focuses on creative samples rather than on how leads will flow from ad to front desk to booked appointment.
- The retainer math has no clear ROI threshold inside 90 days, and the agency dodges the question of when the clinic should fire them.
- They will not put you in touch with two current clients before signing.
How to interpret the red flags
Any one of these on its own is a warning.
Two or more, and the relationship will not produce the revenue that justifies the retainer.
For owners trying to figure out how to pick a marketing agency, these warning signs are often more valuable than any sales presentation. The agencies that create the best outcomes for cash-pay clinics are usually transparent about results, willing to connect you with current clients, and focused on revenue growth rather than marketing metrics that never make it to the bank account.
The cash-pay clinics that have grown the fastest in our portfolio all hired the agency that could pass all five filters.
The clinics that hired around them mostly burned 12 to 18 months before re-hiring.
How much should a cash-pay medical practice expect to pay a marketing agency?
The ROI rule
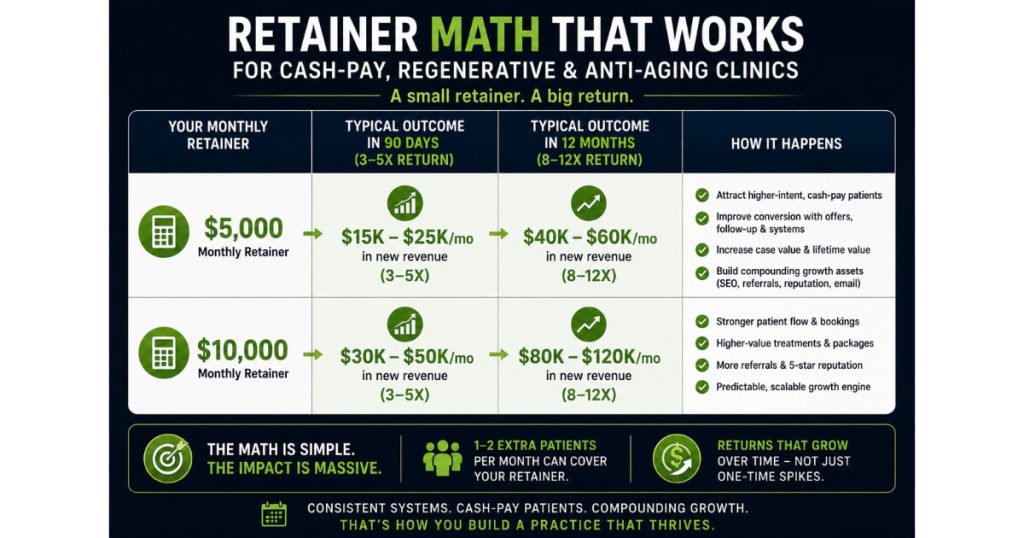
The retainer math depends on revenue level and offer mix, but the rule that scales across verticals is that the agency should produce:
- at least 3 to 5 times their own retainer in additional cash-pay revenue inside 90 days
- 8 to 12 times their own retainer inside 12 months
or the relationship is not worth keeping.
Example: $5K monthly retainer
A $5K monthly retainer should produce:
- $15K to $25K of net new cash-pay revenue in the first 90 days
- $40K to $60K of incremental monthly revenue by month 12
Example: $10K monthly retainer
A $10K retainer doubles those numbers.
The floor and ceiling
Below the floor, the agency is taking margin out of the clinic.
Above the ceiling, the agency is undercharging and the relationship is fragile because they cannot reinvest in headcount to support the account.
The real cost
The retainer is not the cost.
The cost is what the retainer prevents the clinic from doing instead — and a good agency should be obviously paying for itself in the recurring numbers within one quarter, not in some far-off promise about “compounding brand equity.”
What does a clinic owner say about working with Real ADvice?
Nick Wingo, founder and CEO of Awaken IV
Quoting verbatim from the testimonial recorded May 2026:
“When I came to them, my high level was a mess. My leads were going all over the place. I didn’t have any clear system processes. My booking was confusing and I was losing some leads. These guys have been able to really get me squared away and get me back on track.”
What typically changes after implementation
The pattern is consistent across the portfolio.
Owners come in with:
- leads dropping through cracks between channels and the front desk
- no clear CRM logic
- ad spend producing volume that the operations cannot absorb
Inside 60 to 90 days:
- lead routing is tightened
- the CRM is tightened
- the booking flow is tightened
- the front-desk script is tightened
The same ad spend starts producing measurably more booked patients.
What happens six months later
Six months in:
- the membership base has typically grown by 20 to 40 percent
- the owner has stopped being the bottleneck
The work is unglamorous and the results compound.
One regenerative medicine clinic we worked with hit a 79.4% conversion rate from lead to booked appointment without any ad spend — that is what fixing the operational handoff looks like in the numbers.
Should a cash-pay clinic hire one agency for everything or stack multiple specialists?
The short answer
One integrated partner is almost always the right answer for a cash-pay clinic under $10M of annual revenue.
Why
The failure mode at this scale is operational handoff between:
- marketing
- front desk
- sales
- clinical
not creative quality on any single channel.
One integrated partner vs. multiple specialists
A single integrated agency that owns:
- the offer
- the funnel
- the CRM logic
- the front-desk training
- the weekly numbers review
will outperform three specialist agencies that each optimize their own slice.
When the math changes
Above $10M, the math sometimes flips, because the marketing operation is large enough that a specialist on a single channel (TV, radio, programmatic) can pencil out as an additive layer on top of the integrated team.
Below that line:
- the cost of coordination between specialists eats the gain
- the leaks at the handoff between agencies destroy the conversion rate the clinic was trying to buy
The recommendation
Pick the agency that can run the whole stack.
Hold them to the 90-day ROI math.
Add specialists only when the integrated baseline is already producing.
What’s the next step?
If you are a cash-pay medical practice owner interviewing marketing agencies — or thinking about firing one and starting over — the seven-question filter above is the framework.
Book a strategy call and we will walk through it against your specific clinic.
On the call we will pull:
- the named-clients filter
- the lead-routing audit
- the retainer-math sanity check
- the exit-clause sanity check
- the two-current-clients reference call
If we are not the right fit, we will say so on the call.
If we are, we will tell you:
- what the first 90 days look like
- what revenue threshold the engagement needs to clear to keep going
Either way you leave the call with a checklist you can use to interview any other agency you talk to.