How Do I Add a Second Provider to My Cash-Pay Medical Practice?
The fastest way out of the owner-operator ceiling at a cash-pay clinic is to add a second provider and train them properly. Here’s the three-phase training model Real ADvice uses to get a new provider closing consults inside weeks — not months — so you can scale from $1M to $4M without burning out.
When is the right time to add a second provider to a cash-pay clinic?
When the owner-provider’s calendar is consistently booking out 2+ weeks and the practice is leaving consult slots — and revenue — on the table.
If you’re stuck around $1M per year and every additional patient feels like it costs you sleep, you’ve hit the owner-operator ceiling.
The exit isn’t more marketing. It’s another set of hands in the consult room.
A second provider trained the right way unlocks roughly a doubling of capacity within 90 days; a third unlocks the path from $2M to $4M.
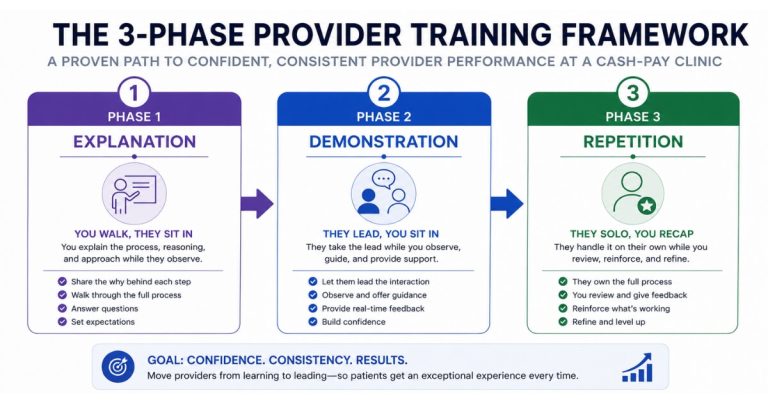
What is the John Wooden Explanation-Demonstration-Repetition training method?
It’s a three-phase training framework that gets a new provider up to speed faster than shadowing alone.
Phase 1 — Explanation
The owner-provider does consults with the new hire sitting in the room.
Phase 2 — Demonstration
The new provider leads consults while the owner sits in.
Phase 3 — Repetition
The new provider runs consults solo and the owner debriefs each day.
The reason it works is the same reason Wooden’s UCLA dynasty worked: the learner sees the standard performed, performs it under observation, then performs it independently with rapid feedback.
No mystery, no guessing.
What does Phase 1 (Explanation) look like in practice?
The owner walks every consult the same way you’ve always walked it, with the new provider physically in the room.
After each consult, the owner explains the choices made:
- Why this offer at this price
- Why the program-not-membership pitch for this patient
- Why the lab order
- Why the close was a “yes” or a “not yet”
This phase usually runs 1–2 weeks.
Done with concentration, it loads the new provider with the playbook before they ever talk.
Done lazily, it produces a new provider who can mimic the script but not improvise.
The difference shows up in close rate at week six.
What does Phase 2 (Demonstration) look like in practice?
The new provider runs the consult.
The owner sits in, mostly silent, only stepping in if the patient is about to walk out or about to be miscoached.
After the consult, the owner debriefs the new provider on:
- What they did well
- The two specific moves they should change on the next consult
Phase 2 runs another 1–2 weeks.
The goal is to let the new provider make small mistakes in front of you, get corrected fast, and not develop bad habits unsupervised.
By the end of Phase 2, the new provider should be closing at 70%+ of the owner’s close rate — that’s the green light to move on.
What does Phase 3 (Repetition) look like in practice?
The new provider runs consults solo.
The owner debriefs them at the end of every day for the first 30 days.
After a month, the debriefs go from daily to weekly.
After two months, the new provider is closing at parity and the owner is mostly running the business, not the consult room.
The fastest learning curves Real ADvice has seen are inside clinics that protect the daily debrief in Phase 3.
The slowest are inside clinics that skip the debrief because “they’re doing fine.”
Without rapid feedback, drift creeps in and the close rate quietly slides 15–20% over a quarter.
How fast can a new provider get up to speed at a cash-pay clinic?
Six to eight weeks for a competent provider with prior clinical experience in the modality; 10–12 weeks for someone newer to the vertical.
The speed at which you’re successful with adding a second provider depends far more on the quality of the training process and feedback loops than on the provider’s credentials alone.
The variable that matters most is feedback loop frequency, not raw IQ.
A daily debrief in Phase 3 cuts the learning curve roughly in half compared with weekly check-ins.
The financial frame: every week shaved off the training timeline is a week of salary the practice paid without a fully-productive provider.
Faster training = faster ROI on the hire = better hire economics across the year.
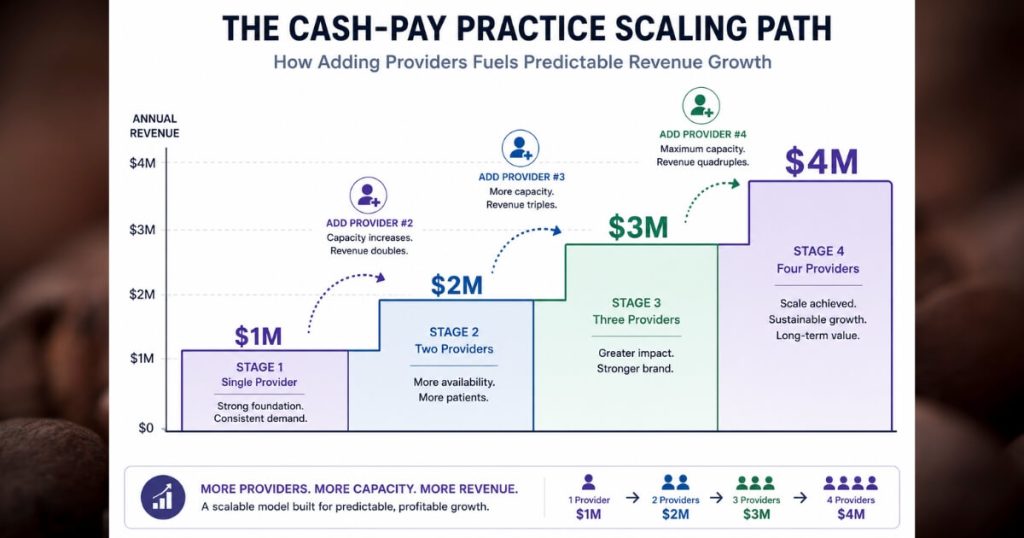
How does adding a second provider scale a cash-pay clinic from $1M to $4M?
Provider capacity is the throttle on a cash-pay clinic’s growth.
Once the owner-provider hits ceiling at ~$1M, every incremental provider adds another $1M–$1.5M of capacity — assuming the new provider closes at near parity and the marketing engine keeps the consult calendar full.
Inside an HRT clinic Real ADvice grew from $1M to $4M with 250 active members paying $1,000/month, the growth path wasn’t a paid-ad miracle.
It was provider capacity, properly trained, with a membership model that compounded retention.
The same math runs through Dr. Joy Kong’s regenerative practice, where Real ADvice helped her hire 4 more doctors and scale herself out of day-to-day operations — proving the framework works across HRT, regenerative, and aesthetic verticals.