How Many Follow-Ups Does It Take to Convert a Cash-Pay Lead (and What to Say)?
Almost every cash-pay clinic loses most of its leads in the same place: the silence after the first call goes unanswered.
The lead requested a neuropathy evaluation, a TRT consult, or a filler offer. The front desk called once, got voicemail, and the lead quietly died in the CRM.
The clinics that scale do the opposite.
They run a structured chase sequence of eight or more touches across call, text, and email.
And they know the exact words for each one.
This is the FAQ on how many follow-ups it really takes to convert a cash-pay lead, what channel each touch should use, when it should fire, and what it should say — pulled from a real multi-touch chase sequence built for a physical medicine and rehabilitation practice.
How many follow-ups does it actually take to convert a cash-pay medical lead?
Plan for at least 8 follow-up touches over two to three weeks before you retire a lead.
Most cash-pay clinics quit after one or two attempts.
That is why their lead-to-appointment rate is poor.
The majority of bookings come from touches three through eight, not the first call.
A lead who requested a neuropathy evaluation, a TRT consult, or a filler offer is not refusing you when they go quiet.
They are busy, distracted, or simply waiting for a reason to act.
Treating a single unanswered call as a “no” is the most expensive mistake a clinic makes.
Why?
Because the lead already raised their hand.
You paid to acquire that intent, and one voicemail does not exhaust it.
The proven structure is a multi-touch chase sequence.
It opens immediately with a voicemail and an email the moment the lead signs up.
Then it layers calls, texts, voicemails, and emails across the next several days.
The cadence looks like this:
- Touch one happens within minutes.
- Touches two through six run every one to three days.
- Touches seven and eight are the persistence-and-breakup pair near the end of the window.
Eight is the floor, not the ceiling.
A $20K neuropathy or regenerative program justifies more contact than a $300 filler offer.
But eight structured touches recover far more revenue than the one-and-done approach almost every clinic defaults to.
The point of a written sequence is that the chase no longer depends on whether a busy front-desk person remembers to follow up.
It runs on rails.
If you want the broader system this sits inside, our patient acquisition framework treats follow-up as part of the funnel, not an afterthought.
What channels should you mix when following up on a cash-pay lead — call, text, or email?
Use all three, but lead with the phone and let email and text carry proof.
The phone call is the primary conversion channel because a cash-pay decision needs a human voice.
That includes:
- Neuropathy therapy
- Hormone programs
- Body contouring
- Regenerative care
- Aesthetic offers
Each channel does a different job.
Email is your proof channel.
It carries success stories, a case-study screenshot, a testimonial video, and the offer details a voicemail simply cannot.
Text is the open-rate channel.
It gets a fast reply when a call goes unanswered and an email sits unread.
And the phone is where the actual conversion happens.
Why?
Because the moment a real person explains the treatment and answers the one objection holding the lead back is the moment the appointment gets booked.

The winning pattern pairs them.
A phone call is backed by a voicemail.
That voicemail is immediately followed by an email or text referencing the same voicemail:
“I just left you a message and sent an email as well.”
The lead sees you across every channel on the same day.
That reads as attentive rather than annoying.
Phone alone gets ignored.
Email alone gets buried.
Text alone feels thin for a four- or five-figure medical decision.
The combination is what moves the unconverted lead from intention to booked appointment.
It is exactly why clinics that generate volume — like the practice in our Eternity Health Partners case study that drives 60 inbound calls a month — pair their inbound demand with a follow-up engine that catches every lead the first call misses.
What should the first follow-up message say to a new cash-pay lead?
Thank them for taking the offer, restate exactly what they signed up for, and ask for a short, specific block of time on the phone.
The first touch should fire within minutes of the opt-in, while intent is highest.
It should be both a voicemail and an email.
The voicemail is short and warm.
It thanks the lead for taking you up on the evaluation.
It says you would love a few minutes to connect personally.
And it repeats your name and number twice so they can actually write it down.
Example:
“This is [Your Name] from Dr. Schwartz’s office at Piedmont Physical Medicine and Rehabilitation. You can reach me at the number on your screen. Again, that is [Your Name].”
Saying the name and number twice sounds excessive.
But remember, the lead is probably driving or distracted.
The repetition is what makes a callback possible.
The email runs longer because it can carry the offer.
It should:
- Restate what the lead requested
- Describe the treatment and the relief it delivers in plain bullets
- Ask for 15 minutes on the phone in the next week
- Close with a P.S. linking to recent success stories
The treatment bullets can include:
- Repair nerve damage
- Walk without pain
- Reduce tingling and numbness
Naming the exact offer the lead raised their hand for matters.
A generic “thanks for your interest” gets deleted.
Specificity proves you remember them.
It also proves this is not a mass blast.
What do you say in the middle follow-up touches when a lead has gone quiet?
Switch from asking for time to delivering proof and social proof.
By the third or fourth touch, the lead has not refused you.
They simply have not had a reason to call back yet.
So your job is to give them one.
A high-performing middle-touch script opens with:
“I was talking with [a patient who got great results] and your name came to mind.”
It is curiosity-driven and human rather than salesy.
It gives you a natural reason to reconnect.
And it does not sound like another “just checking in” message.
The voicemail version names the result the other patient got.
That plants a concrete outcome in the lead’s mind without pitching anything.
From there, the touches escalate the proof.
One voicemail says:
“I have a case study you’ll want to see. It shows how we helped a patient improve their neuropathy pain and symptoms.”
The email that backs it up goes further.
It includes an actual screenshot of a patient and their testimonial.
It also includes a line like:
“As you can see, [Patient] has seen phenomenal results. Click here to watch the video and read the case study.”
The point of touches three through six is to stop chasing and start demonstrating.
You are no longer asking the lead to give you 15 minutes as a favor.
You are showing them that patients exactly like them got the outcome they came looking for.
Proof in the middle of the sequence is what re-engages a cold lead.
Why?
Because it answers the silent objection before the lead has to ask it:
“Does this actually work?”
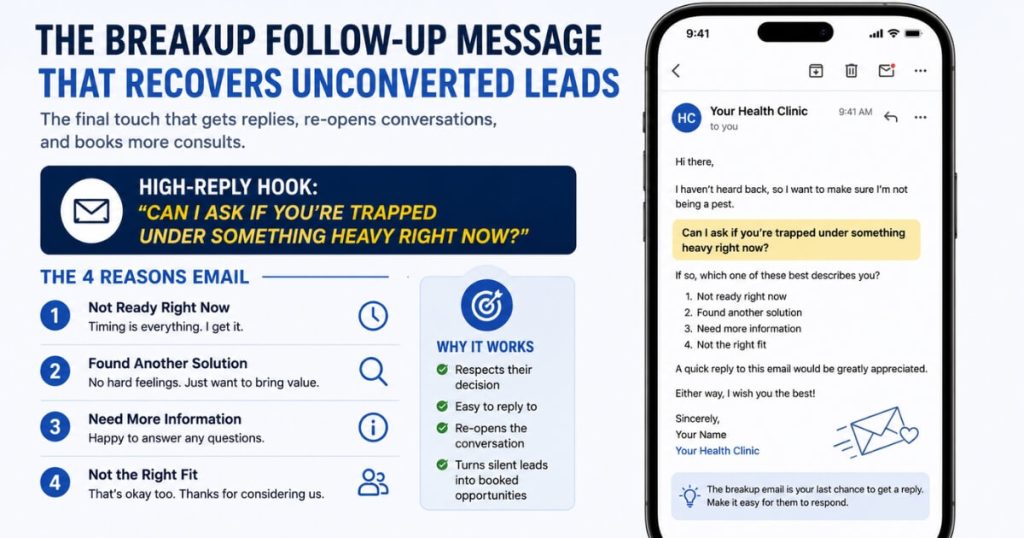
How do you write the final “breakup” follow-up — and does it really work?
The breakup is the touch that gives the lead permission to be done.
It is often the highest-replying message in the entire sequence.
Near the end of the window — touch seven and touch eight — you change the tone from persistence to graceful exit.
The persistence touch is honest and a little vulnerable:
“I’ve been reaching out to you for a while telling you about our services. I know you’re busy — in fact, I am too. The reason I’m so adamant we speak is that I truly believe our services give patients the best chance at finding relief.”
That reframes the chase as conviction rather than desperation.
That distinction matters to a patient who is hesitating.
The breakup that follows acknowledges the silence directly:
“I’m concerned that I’ve offended you with my persistence. If so, I apologize. It could be that you no longer suffer from the pain, or that you are seeking treatment elsewhere — and if that’s the case, I’m sorry I missed the opportunity. But if you are still looking for a solution, give me a call.”
A lighter, high-reply email variant lists the four reasons the lead might be ignoring you.
One of those reasons can be the joke that they are “trapped under something heavy and cannot reach the phone.”
Then it asks them to reply with which one it is.
Breakups work because the fear of losing the relationship triggers a response that another polite check-in never would.
A surprising share of recovered bookings come from this very last message.
That is the strongest argument there is for never stopping at touch one.
How fast does the first follow-up need to go out — and how long should the whole sequence run?
Send touch one within minutes of the opt-in.
Then run the full eight touches across roughly two to three weeks.
Speed-to-lead is the single biggest lever in the whole sequence.
A lead contacted in the first five minutes converts at a multiple of one contacted hours later.
The reason is simple.
You reach the lead while the intent that made them fill out the form is still hot.
Wait until the next business day and you are now competing with every other thought that has entered their head since.
You are also competing with any clinic that called faster.
The immediate voicemail-and-email pair is not a courtesy.
It is the highest-leverage moment in the entire chase.
After that, space the sequence so it stays present without becoming noise.
A strong cadence includes:
- An immediate voicemail-and-email pair
- A phone call without voicemail in the first few days
- A separate voicemail follow-up
- An email-plus-voicemail proof pair mid-sequence
- A persistence touch
- A breakup touch
Two to three weeks is the right total window for most cash-pay offers.
It is long enough to outlast a busy patient’s distraction.
It is short enough that the intent has not gone fully cold.
The mistake is almost never the length of the sequence.
It is the gap.
Clinics lose the lead in the silence between touch one and a follow-up that never comes.
The entire purpose of a written, channel-mixed cadence is to make sure that silence never happens.
FAQ’s About Lead Follow-Up Cadence
How many follow-ups does it actually take to convert a cash-pay medical lead?
Plan for at least 8 follow-up touches over two to three weeks before you retire a lead.
Most cash-pay clinics quit after one or two attempts.
That is why their lead-to-appointment rate is poor.
The majority of bookings come from touches three through eight, not the first call.
A lead who requested a neuropathy evaluation, a TRT consult, or a filler offer is not refusing you when they go quiet.
They are busy, distracted, or waiting for a reason to act.
The proven structure is a multi-touch chase sequence.
It opens immediately with a voicemail and an email the moment they sign up.
Then it layers calls, texts, voicemails, and emails across the next several days.
Touch one happens within minutes.
Touches two through six run every one to three days.
Touches seven and eight are the persistence-and-breakup pair near the end of the window.
Eight is the floor, not the ceiling.
High-ticket programs justify more.
But eight structured touches across call, text, and email recover far more revenue than the one-and-done approach almost every clinic defaults to.
What channels should you mix when following up on a cash-pay lead — call, text, or email?
Use all three, but lead with the phone and let email and text carry proof.
The phone call is the primary conversion channel because a cash-pay decision needs a human voice.
That includes neuropathy therapy, hormone programs, and body contouring.
Email is your proof channel.
It carries success stories, a case-study screenshot, a testimonial video, and the offer details a voicemail cannot.
Text is the open-rate channel.
It gets a fast reply when a call goes unanswered and an email sits unread.
The winning pattern pairs them.
A phone call is backed by a voicemail.
Then it is immediately followed by an email or text referencing that same voicemail.
That way, the lead sees you across every channel in the same day.
Phone alone gets ignored.
Email alone gets buried.
Text alone feels thin for a four- or five-figure medical decision.
The combination is what moves the unconverted lead from intention to booked appointment.
What should the first follow-up message say to a new cash-pay lead?
Thank them for taking the offer, restate exactly what they signed up for, and ask for a short, specific block of time on the phone.
The first touch should fire within minutes of the opt-in, while intent is highest.
It should be both a voicemail and an email.
The voicemail is short and warm.
Thank them for taking you up on the evaluation.
Say you would love a few minutes to connect personally.
Repeat your name and number twice so they can write it down.
The email runs longer because it can carry the offer.
Restate what they requested.
Describe the treatment and the relief it delivers in plain bullets.
Ask for 15 minutes on the phone in the next week.
Then add a P.S. linking to recent success stories.
Naming the exact offer they raised their hand for matters.
A generic “thanks for your interest” gets deleted.
Specificity proves you remember them.
What do you say in the middle follow-up touches when a lead has gone quiet?
Switch from asking for time to delivering proof and social proof.
By the third or fourth touch, the lead has not refused you.
They simply have not had a reason to call back yet.
So give them one.
A high-performing middle-touch script opens with:
“I was talking with [a patient who got great results] and your name came to mind.”
That line is curiosity-driven and human rather than salesy.
The next touches escalate the proof.
One can say:
“I have a case study you’ll want to see.”
Then follow it with an email containing:
- A screenshot of a patient testimonial
- A link to the video
- A link to the case study
The point of touches three through six is to stop chasing and start demonstrating.
You are no longer asking the lead to give you 15 minutes as a favor.
You are showing them that patients exactly like them got the outcome they came looking for.
Proof in the middle of the sequence is what re-engages a cold lead.
How do you write the final “breakup” follow-up — and does it really work?
The breakup is the touch that gives the lead permission to be done.
It is often the highest-replying message in the entire sequence.
Near the end of the window, touch seven and touch eight change the tone from persistence to graceful exit.
The persistence touch is honest:
“I’ve been reaching out for a while because I truly believe our services give patients the best chance at relief.”
The breakup that follows acknowledges the silence directly:
“I’m concerned I’ve offended you with my persistence — if so, I apologize. It could be you no longer have the pain, or you’re being treated elsewhere. But if you’re still looking for a solution, call me.”
A lighter, high-reply variant lists the four reasons they might be ignoring you.
That can include the joke that they are “trapped under something heavy and cannot reach the phone.”
Then ask them to reply with which one it is.
Breakups work because the fear of losing the relationship triggers a response that another polite check-in never would.
Many recovered bookings come from this last message.
How fast does the first follow-up need to go out — and how long should the whole sequence run?
Send touch one within minutes of the opt-in.
Run the full eight touches across roughly two to three weeks.
Speed-to-lead is the single biggest lever in the whole sequence.
A lead contacted in the first five minutes converts at a multiple of one contacted hours later.
Why?
Because you reach them while the intent that made them fill out the form is still hot.
After that immediate first touch, space the sequence so it stays present without becoming noise.
Use a phone-call-without-voicemail and a voicemail in the first few days.
Use an email-plus-voicemail proof pair mid-sequence.
Then use the persistence and breakup touches in the back half.
Two to three weeks is the right total window for most cash-pay offers.
It is long enough to outlast a busy patient’s distraction.
It is short enough that the intent has not gone fully cold.
The mistake is not the length.
It is the gap.
Clinics lose the lead in the silence between touch one and a follow-up that never comes.