How Do You Handle Price Objections on a GLP-1 Weight-Loss Consult at a Cash-Pay Clinic?
Price objections on a cash-pay GLP-1 consult almost never mean the patient cannot afford it.
They mean the value is not obvious yet, or the patient does not believe the program will actually work for them.
The clinics that close at $399 — and then upsell into a $300 to $1,000 a month membership — do not win the call by defending the number or discounting it.
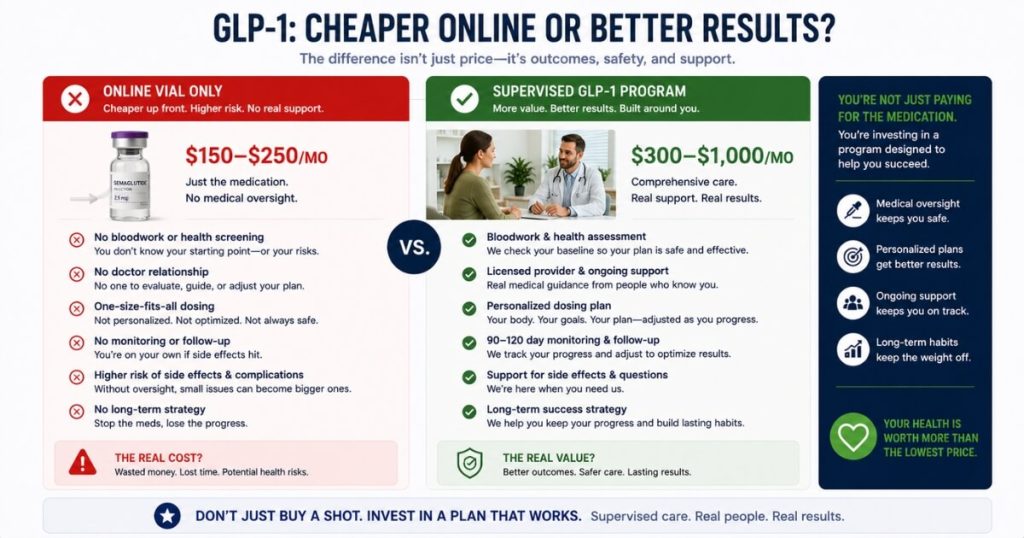
They win by anchoring the price against the real value, separating supervised care from a cheaper online vial, and reframing the spend as an investment in finally keeping the weight off.
This is the field-tested playbook for handling “it’s too expensive” and “I can get it cheaper online,” pulled from the GLP-1 consult and lead-nurture scripts we run for cash-pay weight-loss clinics, with the exact words to say at each step.
Is the GLP-1 price objection really about money?
Almost never.
“It’s too expensive” is usually code for “I’m not convinced this will work for me” or “I don’t trust that I’ll get my money’s worth.”
People who are certain a $399 program will solve a problem they have spent years and thousands of dollars failing to fix do not call it expensive.
They call it a bargain.
The patient on the other end of a GLP-1 consult has almost always already spent real money on diets, programs, coaches, and gym memberships that did not stick.
So when price comes up, do not negotiate the number.
Go back to belief.
Ask what they have already tried and what it cost them.
Then reframe the GLP-1 program as the thing that finally makes all of that prior spend pay off.
This is why the consult script asks:
“What else have you tried recently to lose the weight?”
It asks that before it ever quotes a price.
That answer is your ammunition.
When the patient later says $399 is a lot, you remind them they have already spent more than that on things that failed.
And this is the supervised, lab-based program built so the weight stays off.
Price objections collapse when value is obvious.
They harden when you defend the number.
If you want the full patient-acquisition system that feeds these consults, start with our patient acquisition strategy for cash-pay clinics.

How do you anchor the price so $399 feels like a deal?
State the real, full value of the bloodwork and consult first.
Then present the offer as a discount off it.
The line that works, almost verbatim from the script:
“The investment for the comprehensive bloodwork and the initial doctor consult is usually $750. For patients focused specifically on weight loss right now, we’re offering that same level of care for $399. If you’re local, you can come straight to the clinic to have your bloodwork done and skip the line at your local lab.”
Now $399 is measured against $750, not against zero.
The patient is not deciding whether to spend $399 out of nowhere.
They are deciding whether to take $750 of care for $399.
Layer a second anchor on top.
The monthly membership runs $300 to $1,000 depending on what the labs show.
So when you walk the patient through the three steps, the $399 entry point is plainly the smallest number in the whole conversation.
Those three steps are:
- Comprehensive bloodwork
- A doctor consult to review it
- A personalized membership plan
Always name the big number before the small one.
Anchoring is not a trick.
It is giving the patient an honest reference point so the price lands in context instead of in a vacuum.
A clinic that does this consistently is part of how NuLevel Wellness Medspa added 3,727 new patients and $6.7M a year.
The offer was anchored, and the consult closers knew the order to say the numbers in.
What do you say when a patient says they can get GLP-1 cheaper online?
Agree first.
Then separate the molecule from the medicine.
Never argue that the patient is wrong about the price.
They are not.
Fighting it makes you sound defensive and makes the cheap option more attractive.
Instead, concede the point and immediately redraw the comparison:
“You’re right, you can find it cheaper online — and if the goal was just to get a vial of semaglutide shipped to your door, I’d honestly tell you to do that. But that’s not what you called about. You called because the last few things you tried didn’t keep the weight off.”
Then itemize what they are actually buying:
“What you’re paying for here is comprehensive bloodwork, a doctor who reads it and tells you why you’ve been stuck, a dosed plan built on your actual labs, and someone watching your progress for the next 90 to 120 days. The big telehealth companies skip all of that — they just ship the drug. We do this in a responsible, supervised way so you keep the weight off for good, not just lose it and bounce back.”
The cheaper-online product and the supervised-program product are not the same thing.
The patient already suspects that.
That is precisely why they booked a consult instead of just buying online.
Your job is to name the difference out loud.
Should you offer a payment plan on a GLP-1 consult?
Use it as a close on a real objection, not as your opening offer.
Leading with a payment plan signals that the price is soft.
It invites more pushback.
The patient hears “this is negotiable” and starts negotiating.
Hold it in reserve.
When a genuinely interested patient hits a real cash-flow wall, that is when you deploy it.
This should be a patient who has agreed they are a candidate and wants the outcome.
Use:
“The total today to get started is $399. If splitting that makes it easier to begin this week instead of waiting, we can break it into payments — what matters is that you start.”
That moves the conversation off whether and onto when.
That is exactly where you want it.
Notice that the membership itself is already a monthly structure.
It runs $300 to $1,000 a month.
So most of the affordability story is built into the model before payment plans even come up.
The $399 entry is the only lump the patient has to clear.
That is why a split on that one number is such a clean final move.
It removes the last barrier without cheapening the program.
It also avoids training the patient to expect discounts on everything that follows.
How do you reframe the GLP-1 price as an investment instead of a cost?
Tie the spend to the outcome and the timeline.
Then put the patient’s own goal weight inside the sentence.
A cost is money that leaves.
An investment is money that returns.
Make the patient feel the return:
“You told me you want to lose 40 pounds and keep it off. When patients work with us, we expect them to hit their weight-loss goal in 90 to 120 days, assuming the bloodwork says they’re a good candidate. So the question isn’t whether $399 is a lot of money — it’s whether finally losing those 40 pounds and keeping them off is worth getting started this week.”
That converts an abstract number into a concrete result the patient has already told you they want.
The script frames the number this way on purpose.
Members invest between $300 and $1,000 a month to reach their goals.
The word invest is doing real work.
An investment implies a return.
A cost does not.
The same logic powers recurring-membership clinics like Eternity Health Partners, which built 250 members paying $1,000 a month.
Patients who view the monthly spend as an investment in an outcome stay enrolled far longer than patients who view it as a bill.
Frame it as a return from the first consult and the retention follows.
When in the call should price come up?
After value is established, never before.
The entire GLP-1 consult is engineered to earn the right to quote a price.
Before naming a number, you ask:
- How much they want to lose
- What they have already tried
- Why it did not work
- Whether they have had recent bloodwork
- Whether they feel ready to lose the weight in the next three to four months
By the time price comes up, the patient has talked themselves into wanting the outcome.
That is the entire game.
If a patient asks “how much does it cost?” too early, do not blurt the number.
Give a soft range and steer back to candidacy:
“Most members invest between $300 and $1,000 a month depending on their labs — but let me make sure this is even right for you first, because I don’t want you spending money on something that won’t work.”
That answer respects the question.
It also demonstrates that you are screening for fit rather than just selling.
And it buys you the time to build value before the firm $399 quote lands.
Quoting price into a vacuum is the single most common reason a cash-pay GLP-1 consult dies.
Build the value, confirm candidacy, then quote.
In that order, every time.
FAQ’s About Handling Price Objections on GLP-1 Consults
Is the GLP-1 price objection really about money?
Almost never.
“It’s too expensive” is usually code for “I’m not convinced this will work for me” or “I don’t trust that I’ll get my money’s worth.”
People who are certain a $399 program will solve a problem they have spent years and thousands of dollars failing to fix do not call it expensive.
They call it a bargain.
So when price comes up, do not negotiate the number.
Go back to belief.
Ask what they have already spent on diets, programs, and gym memberships that did not stick.
Then reframe the GLP-1 program as the thing that finally makes all of that prior spend pay off.
Price objections collapse when value is obvious.
They harden when you defend the number.
How do you anchor the price so $399 feels like a deal?
State the real, full value of the bloodwork and consult first.
Then present the offer as a discount off it.
The line that works:
“The investment for the comprehensive bloodwork and the initial doctor consult is usually $750. For patients focused specifically on weight loss right now, we’re offering that same level of care for $399.”
Now $399 is measured against $750, not against zero.
Layer a second anchor on top.
The monthly membership runs $300 to $1,000 depending on what the labs show.
So the $399 entry point is plainly the smallest number in the whole conversation.
Always name the big number before the small one.
Anchoring is not a trick.
It is giving the patient an honest reference point so the price lands in context instead of in a vacuum.
What do you say when a patient says they can get GLP-1 cheaper online?
Agree.
Then separate the molecule from the medicine.
Say:
“You’re right, you can find it cheaper online — and if the goal was just to get a vial of semaglutide shipped to your door, I’d tell you to do that. But that’s not what you called about. You called because the last few things you tried didn’t keep the weight off. What you’re paying for here is comprehensive bloodwork, a doctor who reads it and tells you why you’ve been stuck, a dosed plan built on your actual labs, and someone watching your progress for the next 90 to 120 days. The big telehealth companies skip all of that — they just ship the drug. We do this in a responsible, supervised way so you keep the weight off for good, not just lose it and bounce back.”
The cheaper-online product and the supervised-program product are not the same thing.
The patient already suspects that.
That is why they booked a consult instead of just buying online.
Should you offer a payment plan on a GLP-1 consult?
Use it as a close on a real objection, not as your opening offer.
Leading with a payment plan signals the price is negotiable.
It invites more pushback.
Hold it in reserve.
When a genuinely interested patient hits a cash-flow wall, deploy it:
“The total today to get started is $399. If splitting that makes it easier to begin this week instead of waiting, we can break it into payments — what matters is that you start.”
That moves the conversation off whether and onto when.
The membership itself is already a monthly structure.
It runs $300 to $1,000 a month.
So most of the affordability story is built into the model.
The $399 entry is the only lump the patient has to clear.
A split on that one number removes the last barrier.
How do you reframe the GLP-1 price as an investment instead of a cost?
Tie the spend to the outcome and the timeline.
Use the patient’s own goal weight in the sentence.
“You told me you want to lose 40 pounds and keep it off. When patients work with us, we expect them to hit their weight-loss goal in 90 to 120 days, assuming the bloodwork says they’re a good candidate. So the question isn’t whether $399 is a lot of money — it’s whether finally losing those 40 pounds and keeping them off is worth getting started this week.”
That converts an abstract price into a concrete return.
The script even frames the number this way on purpose.
Members invest between $300 and $1,000 a month to reach their goals.
The word invest is doing work.
An investment has a return.
A cost does not.
When in the call should price come up?
After value is established, never before.
The whole GLP-1 consult is built to earn the right to quote a price.
You ask how much they want to lose, what they have already tried, why it did not work, and whether they feel ready to lose the weight in the next three to four months before you ever name a number.
If a patient asks “how much does it cost?” early, give a soft range and steer back:
“Most members invest between $300 and $1,000 a month depending on their labs — but let me make sure this is even right for you first, because I don’t want you spending money on something that won’t work.”
Quoting price into a vacuum is the single most common reason a cash-pay GLP-1 consult dies.
Build the value, confirm candidacy, then quote.