Google & YouTube Ads for Cash-Pay Medical Practices — From Tight Phrase Match to Performance Max (and How to Build YouTube Video Assets That Don’t Waste Money)
Google and YouTube ads are the highest-intent paid channel a cash-pay medical practice can run — patients are literally typing in the treatment they want, then clicking. They also carry tricky policies and a higher cost per lead than Facebook or TikTok, so the structure matters. The play that works across the 40 fastest-growing cash-pay clinics we’ve helped scale: start tight phrase match, get data, then graduate to Performance Max and build YouTube assets from what people are actually searching. Here’s the FAQ on the full progression — what to launch on day one, when to expand, and how to avoid burning money on the wrong video creative.
Why do Google and YouTube ads typically produce higher-intent leads than Facebook for a cash-pay medical practice?
Direct answer: Because Google and YouTube ads intercept patients who are actively searching for the treatment — that intent layer doesn’t exist on Facebook, which is interruption-based, and it shows up downstream as a higher conversion rate and a sales team that doesn’t burn out.
On Facebook and Instagram:
- The patient is scrolling
- The ad interrupts
- The offer has to do all the work
That’s why aggressive offers and fast follow-up are non-negotiable on Meta, and why most of the time you need cash in as fast as you’re putting it out.
On Google and YouTube:
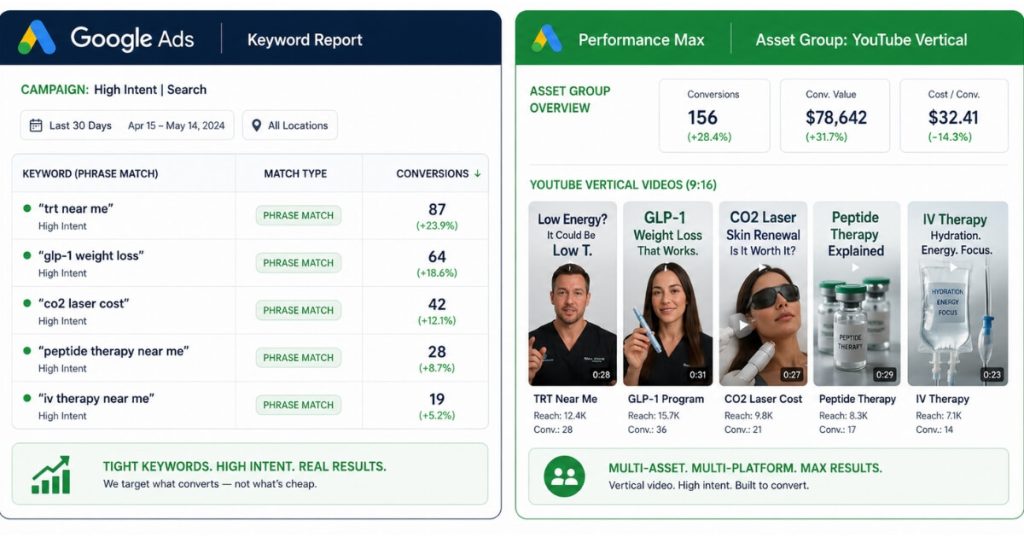
- The patient typed “TRT near me”
- Or “GLP-1 weight loss”
- Or “CO2 laser cost”
…into the search bar.
They self-identified as solution-aware before they ever saw your ad. That single behavioral difference changes everything downstream.
The tradeoff is real:
- Google’s cost per lead is typically higher than Facebook’s or TikTok’s
- The policies are tricky to navigate (especially for regenerative, peptides, and anything FDA-questionable)
But:
- The conversion rate is higher
- Lead quality is higher
- The sales team burns out less
They’re not chasing curiosity clicks — they’re talking to people who already raised their hand for the specific treatment.
For a cash-pay medical practice trying to build a durable patient-acquisition engine, that quality difference matters more than the CPL gap.
Which cash-pay medical offers work best on Google and YouTube (and why solution-aware terms convert)?
Direct answer: Anything patients are solution-aware of — GLP-1, TRT, botox, filler, CO2, body contouring, hormone replacement — converts well on Google and YouTube, because they’re searching for the treatment by name.
The Stages of Awareness framework explains why.
People buy when they’re Most Aware.
Google and YouTube reach:
- Product Aware patients
- Most Aware patients
They already know the category. They’re choosing who to buy from.
GLP-1 and TRT have fully moved into Product Aware in 2026:
- The population knows what they are
- Patients are shopping providers
Botox, filler, and CO2 have been Product Aware for years.
If a patient is searching the treatment by name, the click is closer to the buying decision than any equivalent click on Facebook.
That’s also why Problem Aware categories — gut health, chronic fatigue, vague “wellness” — convert worse on Google search than on:
- YouTube education videos
- SEO articles
- Organic social
For Problem Aware audiences, the patient doesn’t know what to type.
For Solution Aware audiences:
- They know exactly what to type
- Your ad needs to be there when they do
The fastest way to know if your offer belongs on Google is to ask:
Would a stranger know to search for this by name?
If yes, it belongs here.
How should a cash-pay medical practice launch a Google Ads campaign (tight phrase match first)?
Direct answer: Start with tight phrase match on the terms you already know patients search for. Don’t open up to broad match. Don’t launch Performance Max on day one. Get data first, then expand.
Tight phrase match is the discipline that protects budget while Google’s auction figures out who your patient actually is.
Pick the 10–30 terms you’re confident your ideal patient types in:
- “trt clinic near me”
- “glp-1 weight loss program”
- “co2 laser cost [city]”
- “botox specials [city]”
Run them as phrase match (in quotes), not broad.
Phrase match still allows search-term variation, so you’ll harvest related queries you didn’t think of, but the variation is constrained enough that you’re not paying for “free weight loss tips” when you’re trying to sell a $1,500 GLP-1 program.
The other discipline at launch:
- One campaign
- One budget
- One geography
Don’t fragment $1,000/month across six campaigns at $150 each — the auction needs density to find your converter.
Run one campaign at $1,000–$2,000/month.
Let it accumulate 30–60 days of search-term data.
Then use that data to make the next decision.
We’ve built this exact launch sequence for a regenerative cash-pay clinic that produced $309,590 in revenue in 10 months while maintaining a 79.4% lead-to-booked conversion rate — the proof that high-intent search converts when the funnel underneath it is clean.
When should I switch from tight phrase match to Performance Max for my cash-pay medical practice?
Direct answer: Switch (or more accurately, expand into) Performance Max once your tight phrase-match campaign has 30+ conversions in the last 30 days and a stable cost per lead — that’s the point where Google’s bidder has enough signal to optimize a broader campaign.
Performance Max takes your conversion data and uses it to find more of the same patient across:
- YouTube
- Display
- Discover
- Gmail
- Search
This progression—from tightly controlled search campaigns to broader machine-learning distribution—is the foundation of Google and YouTube ads from phrase match to Performance Max. The goal isn’t to replace search with automation; it’s to use search data first, then let Google expand into adjacent audiences after the algorithm has learned exactly who your ideal patient is.
It only works if you’ve already trained the algorithm with clean conversion data — which is exactly what tight phrase match is designed to produce.
Launch PMAX with no data and Google’s bidder will spray your budget across audiences that don’t convert.
Launch PMAX with 60 days of clean phrase-match conversions and PMAX will replicate that patient profile at scale.
The right structure once you graduate:
- Keep the tight phrase-match search campaign running
- Add PMAX as the second campaign
Phrase match remains your highest-intent traffic.
PMAX captures:
- YouTube views
- In-market display
- Search variations your keyword list doesn’t cover
Add assets to PMAX:
- Headlines
- Descriptions
- Images
- Especially video assets
That allows PMAX to deliver across YouTube and not just Search and Display.
The two campaigns work together:
- Phrase match = surgical strike
- PMAX = territory expansion
How do I build YouTube video assets without wasting money on the wrong creative?
Direct answer: Don’t guess your video creative upfront. Let your tight phrase-match search-term data tell you what to film — make video assets based on the exact language patients are typing in.
The mistake most cash-pay clinics make is:
- Hiring a video crew before launching ads
- Filming six glossy brand spots
- Wondering why none of them convert when uploaded as PMAX video assets
The cheaper, smarter sequence:
- Run tight phrase match for 30–60 days
- Pull the search-term report
- Identify the top 10 actual queries that produced conversions
- Write a 30–60 second video script for each one
Now your video answers the literal question the patient typed in:
- “what does TRT cost”
- “how fast does GLP-1 work”
- “is CO2 laser painful”
…instead of saying:
“welcome to our beautiful clinic.”
The production bar for YouTube assets is lower than most clinics think.
What works:
- Vertical phone-shot video
- Provider on camera
- Good lighting
- Captions burned in
- The patient’s exact search phrase used as the on-screen hook in the first three seconds
Five to ten of these uploaded as PMAX video assets will typically outperform one $5,000 brand spot, because each one is anchored in a real query that already converted.
The search-term data is your creative brief — use it.
What KPI matters most on Google Ads for a cash-pay medical practice (cost per lead)?
Direct answer: Cost per lead is the KPI to optimize against on Google. Lead quality is generally high enough that the sales process can be fixed over time if the CPL is right.
This is a different optimization target than Facebook, where:
- Cost per schedule
- Cost per attended consult
…matter more than cost per lead.
On Google, the intent layer is doing the quality work for you — the lead came in because they searched the treatment by name.
So the lever you control is CPL:
- Bid management
- Keyword tightness
- Ad copy
- Landing page conversion rate
- Negative-keyword maintenance
Pull CPL down by 30–40% over the first 60 days and the rest of the funnel takes care of itself.
The corollary:
Don’t kill a Google Ads campaign because the close rate from the consult is weak.
That’s a sales-process problem, not a Google Ads problem.
The Google Ads question is:
“Are we paying the right price for the right kind of lead?”
If yes:
- The sales side gets coached
If no:
- The campaign gets restructured
Conflating the two leads to clinics shutting down profitable Google campaigns because their new patient coordinator is undertrained — which costs them dramatically more than fixing the coordinator would.
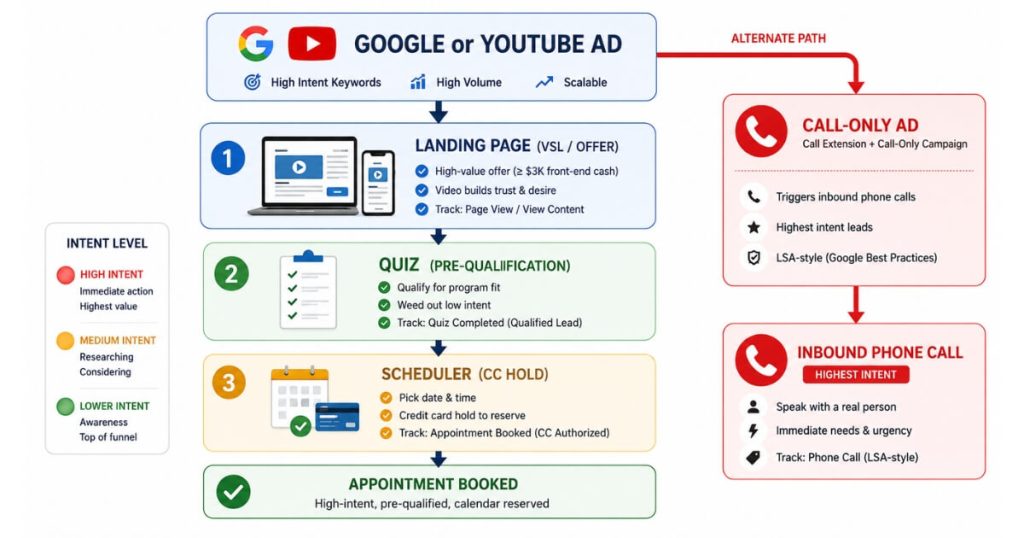
What’s the right funnel for Google Ads at a cash-pay medical practice (landing page → quiz → scheduler with credit-card hold → call-only ads for highest intent)?
Direct answer: The default funnel is ad → landing page (so you can track conversions) → quiz (if you want more quality) → scheduling page with a credit-card-hold field. For the highest-intent traffic, run call-only ads — which is essentially what Google Local Services Ads (LSAs) are.
The landing page exists primarily so you can track conversions cleanly in Google Ads.
You can’t optimize what you can’t measure.
A landing page with a defined goal event is the only reliable conversion signal Google’s bidder will optimize against.
Add a short quiz between the landing page and the scheduler if you want to upgrade quality further.
The quiz acts as a friction filter that removes tire-kickers.
The scheduler at the bottom should require a credit card to hold the appointment.
The patient is not charged — they’re just reserving the slot.
That single step is the biggest no-show preventer in the cash-pay funnel.
For highest-intent traffic:
- Skip the landing page entirely
- Run call-only ads
The ad IS the call button.
The patient taps it.
The call routes straight to the front desk.
This is what LSAs already are, just packaged as an ad format.
Call-only converts the absolute top of the intent pyramid (“trt clinic near me right now”) at a higher rate than any landing-page funnel can, because there’s no page-load step between intent and conversation.
The catch:
Your front desk has to actually pick up.
Answer rate under 90% kills call-only campaigns faster than anything else.
What’s the next step?
The progression — tight phrase match, get data, expand to Performance Max, build YouTube assets from the search-term report, optimize for cost per lead — is the same sequence we’ve run across 40 of the fastest-growing cash-pay medical clinics in the country.
The funnel discipline underneath it:
- Landing page
- Quiz
- Scheduler with CC hold
- Call-only for highest intent
…is what turns the click into the booked appointment.
If you’d like us to map the full sequence to your practice and the specific treatments you sell, book a free strategy call below.