What’s a Good Cost Per Acquired Patient (and Payback Period) for a Cash-Pay Clinic?
Most cash-pay clinics measure the wrong number. They chase a low cost per lead, celebrate a cheap cost per schedule, and then wonder why the bank account does not grow. The only acquisition metric that pays your bills is cost per acquired patient. That means what it actually costs to put one paying patient in the chair. The only benchmark that matters is whether the first cash transaction pays that cost back, ideally on day one. This is the concrete answer on target cost per acquired patient, how it differs from cost per schedule and cost per lead, and the payback-period math by ticket size — pulled straight from the field.
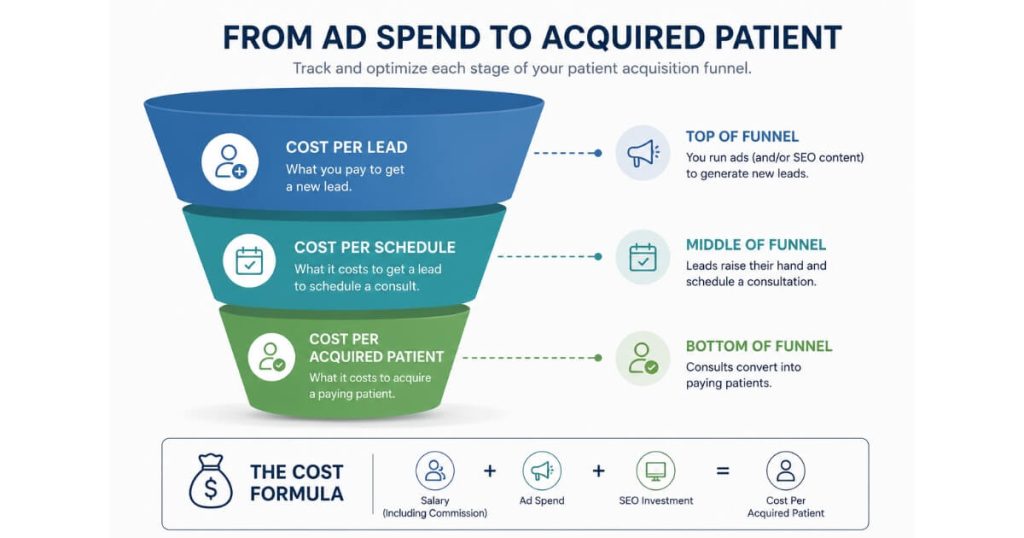
Cost per acquired patient is not cost per lead, and it is not cost per schedule
These are three different numbers measuring three different stages of the same funnel.
Treating them as interchangeable is why most clinics misjudge their marketing.
Cost per lead is the cheapest and least meaningful figure — total spend divided by inquiries.
A low cost per lead means nothing if those leads never book or never show.
Cost per schedule is the next stage.
Take every dollar spent to get appointments booked and divide by the number of new-patient appointments booked that month.
The honest formula is:
Salary + Ad Spend + SEO / total new-patient appointments booked
Cost per acquired patient is the final number.
It is also the only one that pays your bills.
It is total acquisition spend divided by the patients who actually showed up and started paying.
Because attendance is never 100 percent, cost per acquired patient is always higher than cost per schedule.
A $200 cost per schedule at an 80 percent attendance rate is a $250 cost per acquired patient.
Let attendance fall to 50 percent and that same $200 cost per schedule becomes a $400 cost per acquired patient.
The patient who never showed still cost money to book.
You just have to spread that cost across the patients who did.
What counts as acquisition spend (most clinics undercount)
Cost per acquired patient is built from every dollar you spend to turn a stranger into a paying patient — not just the ad account.
You have to include SEO.
Even if you are not running paid ads, you are still spending money to generate those inbound calls.
That money is real.
You have to include the salary, hourly pay, or commission you pay the team that books and confirms appointments.
That labor is part of acquisition.
The complete formula is:
Salary + Ad Spend + SEO, divided by the new patients who actually showed and paid.
There is a second payoff to counting it this honestly.
When your booking team knows that every inbound call cost the business money, they treat each lead with more care.
A lead is not free just because it arrived through organic search.
The team that internalizes that converts better.
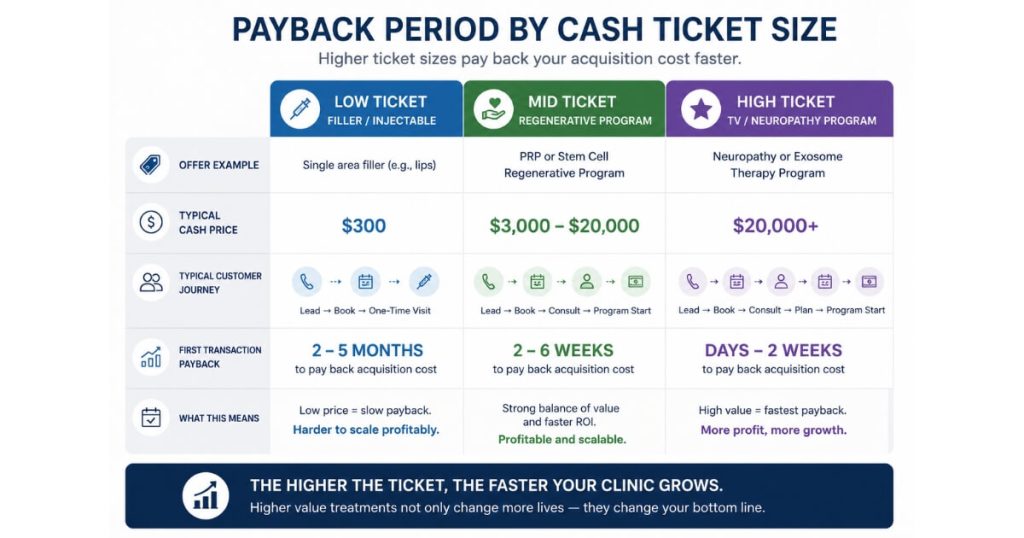
What a good cost per acquired patient actually is — by ticket size
There is no universal dollar figure.
A good cost per acquired patient is defined entirely by your cash ticket and your payback period, not by an industry average.
The benchmark that holds across every cash-pay vertical is a ratio, not a number.
Your first transaction should pay back your cost per acquired patient, ideally several times over.
For a low-ticket front-end offer like a $300 filler appointment, a cost per acquired patient in the low hundreds works.
The patient pays back immediately and lifetime value comes from rebooking.
For a $3,000 to $20,000 regenerative or neuropathy program, a cost per acquired patient of several hundred to a couple thousand dollars is still excellent.
One closed case covers many acquisitions.
For a $20,000-plus program sold off long-form TV, a four-figure cost per acquired patient is normal and profitable.
Stop asking what number is good in the abstract.
Ask whether the first cash transaction from that patient covers the cost to acquire them — and how fast.
The right way to choose the channel and offer for each treatment is covered in our patient acquisition hub.
The payback-period math that keeps a cash-pay clinic solvent
The strongest cash-pay clinics target a payback period at or near zero.
The first transaction covers the cost to acquire the patient on the same visit.
Payback period is the time it takes for the cash a patient pays you to equal what you spent to acquire them.
The math is one line:
Cost per acquired patient divided by the cash collected on the first transaction
If it costs $250 to acquire a patient and they pay $500 on the first visit, your payback period is half of one transaction.
You doubled your money on day one.
If it costs $1,500 to acquire a $20,000 neuropathy patient, you are paid back many times over the moment they enroll.
The danger zone is when payback stretches across multiple visits.
On high-ticket front-end offers, the cash needs to come in as fast as you are putting it out.
A clinic running aggressive paid acquisition on a program that only pays back after the third appointment is financing its own growth out of pocket.
It is also one slow month away from a cash crunch.
Attendance rate is the hidden multiplier on your number
Attendance rate can quietly double your cost per acquired patient without a single change to ad spend.
That makes it the most overlooked lever in the whole calculation.
Cost per acquired patient equals:
Cost per schedule divided by attendance rate
An 80 percent attendance rate is solid.
If you book 10 new-patient appointments and 7 show, you are at a 70 percent attendance rate.
At a $200 cost per schedule and 80 percent attendance, your cost per acquired patient is $250.
Let attendance slip to 60 percent and the same booked appointments now cost $333 per acquired patient.
That is a 33 percent jump in acquisition cost from a problem that has nothing to do with marketing.
This is why attendance rate is the core KPI for lead nurture.
It is also why the best clinics bonus the front-desk team on both new-patient attendance rate and total new patients attended that month.
Fixing attendance is almost always cheaper than buying more leads.
How to lower cost per acquired patient without cutting spend
You lower it by raising the conversion and attendance rates on the leads you already have.
Cost per acquired patient is set as much by your follow-up as by your ad account.
Three levers move it most.
First, lead-to-booked conversion.
A clinic that converts a high share of inquiries into booked appointments spreads its spend across more patients.
That drops the per-patient cost without touching the budget.
Second, attendance rate.
Every point of no-shows you recover lowers cost per acquired patient directly.
That is why an 80 percent target and bonuses tied to it pay for themselves.
Third, payback speed.
Collecting cash on the first transaction means each acquired patient self-funds the next.
So the same budget acquires more patients over time.
We have watched these levers compound.
When the funnel converts that well, the cost per acquired patient takes care of itself.
The same principle scaled a regenerative pain practice.
Elite Pain Doctors generated $2,095,039 in 10 months on roughly 26 organic leads a month.
A high-ticket program with fast payback does not need cheap leads to be wildly profitable.
FAQ’s About Cost Per Acquired Patient
What is the difference between cost per acquired patient, cost per schedule, and cost per lead?
They measure three stages of the same funnel.
Cost per lead is total spend divided by inquiries.
It is cheap and nearly meaningless if leads do not book or show.
Cost per schedule is Salary + Ad Spend + SEO divided by new-patient appointments booked.
Cost per acquired patient is total spend divided by the patients who actually showed and paid.
Because attendance is never 100 percent, it is always higher than cost per schedule.
A $200 cost per schedule at 80 percent attendance is a $250 cost per acquired patient.
At 50 percent attendance, it becomes $400.
What is a good cost per acquired patient for a cash-pay clinic?
There is no universal number.
It is defined by your ticket and payback period.
Low-hundreds works for a $300 filler offer.
Several hundred to a couple thousand is excellent for a $3,000 to $20,000 program.
A four-figure cost is normal and profitable for a $20,000-plus program off long-form TV.
The benchmark is the ratio.
The first transaction should pay back the acquisition cost, ideally several times over.
What is a good payback period, and how do you calculate it?
Target a payback period at or near zero.
The first transaction covers acquisition on the same visit.
The math is cost per acquired patient divided by cash collected on the first transaction.
Acquire a patient for $250 who pays $500 on day one and you have doubled your money immediately.
Payback that stretches across multiple visits on a high-ticket offer is a cash-flow risk.
How does attendance rate change my real cost per acquired patient?
It is a direct multiplier.
Cost per acquired patient equals cost per schedule divided by attendance rate.
At a $200 cost per schedule, 80 percent attendance gives $250 per patient.
At 60 percent attendance, it gives $333.
That is a 33 percent increase with no change to spend.
An 80 percent attendance rate is solid.
Bonusing the team on attendance is usually cheaper than buying more leads.
What should be included when I calculate cost per acquired patient?
Every dollar spent to turn a stranger into a paying patient.
That includes ad spend, SEO, and the salary, hourly pay, or commission of the team that books and confirms appointments.
Even unpaid inbound calls cost money to generate.
The formula is:
Salary + Ad Spend + SEO divided by new patients who showed and paid
Counting SEO and labor also makes your booking team treat each lead with more care.
How do I lower cost per acquired patient without spending less?
Raise lead-to-booked conversion, raise attendance rate, and speed up payback.
Better conversion spreads spend across more patients.
Recovered no-shows lower the number directly.
First-transaction cash lets each patient self-fund the next.
One orthobiologics practice reached a 79.4 percent lead-to-booked conversion with zero ad spend.
That is proof the funnel, not the budget, sets the number.
What’s the next step?
If you are running a cash-pay medical practice and you are not sure whether your acquisition cost is good, the answer is not in an industry average.
It is in your own ticket size, attendance rate, and payback period.
Calculate cost per acquired patient the honest way:
Salary + Ad Spend + SEO, divided by the patients who showed and paid.
Then check whether the first transaction pays that back.
If it does, you can scale.
But if it does not, the fix is almost always conversion and attendance, not a bigger budget.
If you want someone to run those numbers with you — and tell you exactly where your acquisition cost is leaking — that is the conversation to book.
We will map your cost per acquired patient and payback period live on the call.