Why Did My Concierge Clinic’s Patient Close Rate Suddenly Drop? (The Front-Desk Restructure That Fixes Conversion)
The leads are still coming. The offer hasn’t changed. And yet last month your concierge clinic’s close rate slid from where it should be down into the teens. The instinct is to blame the traffic or the ad spend. Almost always, the real culprits are two things nobody is looking at: the owner’s energy, and how the front desk is structured, paid, and held accountable. Here’s the FAQ on why a close rate drops and the front-desk restructure that fixes it for good.
Why Did My Concierge Clinic’s Close Rate Drop Even Though the Leads Are Fine?
Most of the time it’s energy, not leads — and sales is a transference of conviction you can’t transfer when you’re stretched thin.
When a close rate slides from where it should be down to something like 18% in a month while lead quality holds steady, look at what changed for the people doing the closing. In one concierge clinic, the dip lined up exactly with a week where the owner had less staff support, more tasks piled on his plate, and simply wasn’t as present in the sales process. You cannot transfer conviction to a prospect when you’re running on fumes. The patient feels the difference even if they can’t name it.
So before you tear apart your offer or your traffic, fix the operational load on the person closing. Take the admin and the fires off their plate so they can be fully present for the consult. A close rate is a mirror of the closer’s state — and the closer’s state is usually a function of how much else they’re carrying.
Should I Pay My Concierge Clinic’s Front Desk Hourly or on Commission?
It depends on the role. Pay pure admin and activity-based roles a flat hourly rate with no commission. Reserve salary-plus-commission for a true patient care coordinator who owns acquiring and retaining members.
A front-desk role that’s about answering phones, scheduling, and keeping the day running is an activity job — pay it hourly, somewhere in the $20–$28 range depending on level, and just ask them to do the job well. Bolting commission onto a pure admin role only muddies it. But the moment a role is responsible for the productive outcome — booking discovery calls and retaining members — the incentive structure should change.
That coordinator role wants salary plus commission, because it lets you ask more of them and shifts how they think.
An hourly employee asks “how long can I spend on this?” A salary-plus-commission employee asks “how fast can I finish so I can earn more?”
That single mindset shift is worth more than any script. Match the pay model to whether the job is activity or productivity, and you stop overpaying for the wrong behavior.
An HRT clinic we grew from $1M to $4M a year got there partly by building exactly these accountable, properly-incentivized roles around the owner.
What’s a Good Bonus Structure for a Front Desk That Books Appointments?
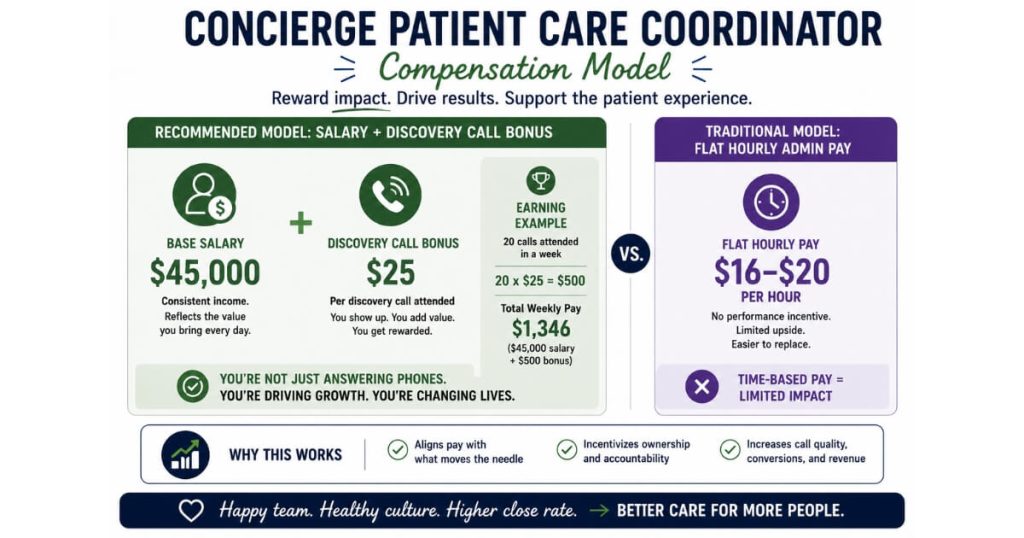
Tie the bonus to the productive outcome — discovery calls attended, not just booked — at roughly $20 to $30 per call on top of base salary.
The key word is attended. If you bonus on calls booked, you incentivize booking calls that never show. Bonus on calls attended and you incentivize the part that actually drives revenue.
A workable model:
- A base of $1,000 to $1,200 a week
- Around $20 to $30 per discovery call attended
- Ten attended calls in a week is an extra $200
For a high-LTV concierge patient, $30 a call is easily justified.
You can layer a team bonus on top to align everyone behind the monthly number. One clinic set it up so hitting $200K in a month paid every eligible team member $300; hitting it by the 20th paid another $300; and hitting 20% above goal paid another $300 — up to $900 per person. Now the whole team is pulling toward the same revenue target instead of optimizing their own little corner.
What Job Title Attracts the Best Front-Desk Hire for a Concierge Clinic?
Post the role as “Executive Administrative Assistant,” not “Patient Care Coordinator” or “Medical Assistant.”
This is a quiet hiring superpower. The soft skills you actually need — organization, presentation, hygiene, composure, and the willingness to have a hard conversation — can’t be taught. People who self-identify as executive administrative assistants already carry those traits, because they’re used to representing a high-net-worth person and being the polished front of an operation. Post an “EA” role and you pull a better demographic and more applications than you’d get advertising a clinical coordinator or MA position.
Screen for fit, not tenure. Be wary of the “lifer” who’s done the same front-desk job for 30 years and is set in their ways, and equally wary of the candidate who’s churned through 17 positions in a few years. The sweet spot is often someone earlier in their career with the right temperament who’s looking to represent something they can be proud of — frequently a 24-to-30-year-old with genuine polish and drive.
Why Did My Front Desk Stop Booking Appointments in Our CRM?
Almost always it’s friction — and the most common culprit is double data entry across two systems.
When a front desk quietly stops booking discovery calls, don’t assume defiance. Go look at the steps. In one clinic the team had stopped booking because every appointment forced them to enter the same patient information twice — once in the practice management system and again in the CRM — and required fields made it slow and painful. They weren’t lazy. They were avoiding a broken process.
The fix is to remove the friction: give them a direct calendar link they can bookmark so the redundant required fields go away, and build an inbound intake form so any lead that needs a discovery call flows straight into the CRM. If the desk is genuinely slammed in the moment, route the lead to the website to self-book rather than losing them. Make the right action the easy action, and booking resumes on its own.
How Do I Hold an Underperforming Front-Desk Employee Accountable?
Start with data, not feelings — track conversion by person — and for chronic problems, put them on a written 60-day performance plan while you hire coverage in parallel.
You can’t coach what you don’t measure. Add tracking for the things that matter:
- Advanced consults booked
- New memberships enrolled
- Separate close rates for each person doing consults, including the owner
When you can say “here’s your conversion versus the target, let’s work on it,” you’re coaching on facts instead of vibes, and the conversation stays professional.
For a chronic issue like lateness or persistent under-performance, escalate cleanly. Consult HR or legal, then deliver a written plan: “I’m giving you 60 days to turn this around,” with specific expectations. And start hiring coverage at the same time — not as a threat, but because hope is not a staffing plan. Use the same framing when you take work off someone’s plate to free them for higher-value work:
“I’m giving you the chance to earn more, and in exchange here’s what I need from you.”
Should I Move My Discovery Calls to a Higher-Priced Paid Consult?
It can be better long-term, but it delays your sales cycle — expect a revenue dip in the transition month, so decide whether to absorb it all at once or phase it in.
A paid advanced consult — say a $650 discovery consult instead of a free call — filters for more serious patients and can raise the quality of who reaches your provider. But there’s a real cost: moving everyone onto the higher-priced model pushed one clinic’s sales cycle out by about two weeks, because patients now schedule further ahead. That two-week stretch shows up as a temporary revenue dip.
So plan for it. Either absorb the dip deliberately as a one-time transition cost, or phase the change in gradually while you keep top-of-funnel full with seminars or other events to refill consults sooner. And protect the price: a $650 consult is only worth $650 if it stays reserved for the discovery call. The moment a team member “helpfully” applies that price to a standard exam, you’ve quietly discounted your own model and stretched the cycle for no reason.
FAQs About Concierge Clinic Front-Desk Conversion
Why Would My Close Rate Drop if My Leads Didn’t Change?
Most often it’s energy and owner bandwidth, not lead quality. Sales is a transference of conviction, and you can’t transfer it when you’re overloaded — a close-rate dip frequently tracks a week where the closer was stretched thin. Fix the operational load before blaming the offer or traffic.
How Should I Pay a Patient Care Coordinator Versus a Front Desk Admin?
Pay pure admin roles a flat hourly rate (about $20–$28) with no commission, and pay a true coordinator who owns acquisition and retention a salary plus commission. The salary-plus-commission model lets you ask more and shifts their mindset from “how long can I spend” to “how fast can I finish to earn more.”
What Bonus Should I Pay Per Appointment Booked?
Bonus on discovery calls attended, not just booked, at roughly $20–$30 each on top of base salary, so ten attended calls is an extra $200 a week. For high-LTV concierge patients, $30 per attended call is easily justified, and a team bonus tied to the monthly revenue goal aligns everyone.
What’s the Best Job Title to Hire a Great Clinic Front Desk?
Post it as “Executive Administrative Assistant” rather than “Patient Care Coordinator.” EA applicants self-select for the soft skills you can’t teach — polish, organization, composure — and you’ll get more applications and a better-fit demographic than advertising a clinical coordinator role.
How Do I Address an Underperforming Front-Desk Employee?
Track conversion and close rate by person so you can coach on facts, and for chronic issues consult HR or legal and put the person on a written 60-day performance plan. Hire coverage in parallel so you’re never dependent on a turnaround that may not happen.
What’s the Next Step?
If your concierge clinic’s close rate dropped and the leads didn’t, the answer is almost never “buy more traffic.” It’s structural: relieve the closer’s operational load, pay each role for the right behavior, hire for soft skills under the right title, remove the CRM friction that quietly kills booking, and hold people accountable with data and a clear plan.
On a strategy call we’ll look at your actual close rates by person, your comp structure, and the friction in your booking process, and tell you exactly what to change first. We’ve rebuilt conversion for clinics across the cash-pay space — including a regenerative clinic that reached a 79.4% conversion rate from lead to booked appointment by tightening exactly these front-desk fundamentals.