How Do You Combine a Discovery Call With Membership Pricing to Close More Patients?
The discovery call and the membership price are not two separate conversations.
They are one sequence, and the order you reveal them in decides whether the patient joins or balks.
Most cash-pay clinics get the call right and then fumble the close. They name the membership number too early. They treat it like a second negotiation. Or they get a verbal yes and let the payment drift off into a text thread that never gets paid.
This is the playbook for using the discovery call to set up the membership price reveal so it lands — anchoring the number, framing the consult fee as a gift the patient gets back, and collecting the commitment on the same call.
It is pulled directly from the field, where the difference between a closed consult and a recurring member usually comes down to one or two sentences.
Should you mention membership pricing on the discovery call or save it for after the patient pays?
Mention it on the discovery call, but frame it as what happens after they get started.
Never frame it as a second price they have to weigh against the first.
The mistake most cash-pay clinics make is treating membership as a separate negotiation.
The discovery call should set the expectation that the entry fee gets them into the practice.
Then, after the consult, you build them a personalized, affordable membership program to stay.
That makes it one path with a natural next step, not two things to sell.
The language that works is simple:
“It’s $600 to get into the practice — that includes your comprehensive lab panel and your initial consult. From that consultation, we’ll put together a personalized, affordable membership program for you that makes sense.”
That single sentence does three jobs:
- It states the entry price plainly, so there is no surprise.
- It frames the membership as personalized and affordable.
- It positions the membership as the outcome of the consult, not a separate sales pitch.
That way, the patient is not bracing for an upsell.
They are expecting a plan.
Save the actual dollar figures for after the consult, when you have a reason to recommend a specific tier.
Naming $199 to $499 a month on a cold call just invites them to shop the number instead of the outcome.
The discovery call is the front door to your whole patient acquisition engine, so the words you choose here set the tone for everything that follows.
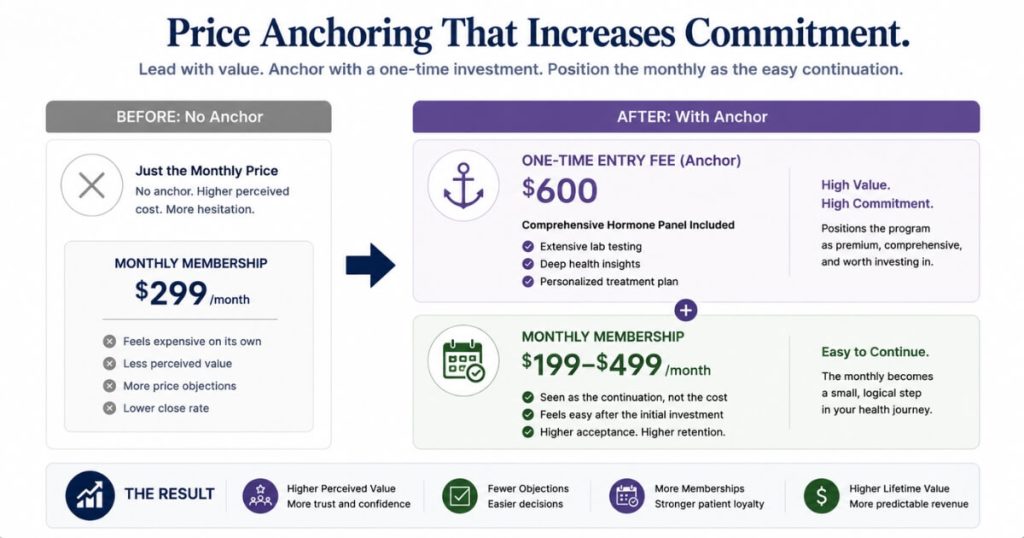
How do you use the discovery call to anchor the membership price so it feels small?
You anchor against the $600 entry fee and the value of the personalized plan.
That way, a $199 to $499 monthly membership reads as the affordable continuation rather than a new expense.
Anchoring is just deciding which number the patient compares the membership to.
If the first number they hear is the membership, they compare it to their other monthly bills.
That makes it feel like a commitment.
If the first number they hear is the $600 to get into the practice, plus the comprehensive lab panel and the doctor’s time, the membership feels different.
It becomes the small, sensible way to keep the results they just paid to discover.
The discovery call is where you set that anchor:
- State the entry investment first.
- Describe the personalized protocol that comes out of the consult.
- Introduce the membership as the way to stay and keep working the plan.
The strongest version of this adds a gift.
Credit the cost of the consult toward the first month’s membership when the patient commits to a 6- or 12-month program.
Now the entry fee is not a sunk cost.
It is a down payment they get back.
The membership feels free for the first month, and the longer commitment is rewarded.
Patients respond to feeling like they are getting something, not losing something.
This is the same anchoring discipline behind clinics like Eternity Health Partners, which built a book of 250 members at $1,000 a month.
The number lands because the value is established before the price is.

What is the credit-back framing and why does it convert discovery calls into members?
The credit-back framing takes the money the patient already spent on the consult and credits it toward their first month’s membership.
That happens when they commit to a 6- or 12-month program.
It converts because it changes the emotional math of the decision.
Without it, the patient sees the $600 entry fee and the monthly membership as two separate hits to their wallet.
With it, the entry fee becomes the first installment of the relationship.
It is refunded into the thing they are about to buy.
That makes it feel like a gift rather than a second charge.
The script is:
“It’s $600 to join the practice, and the cost of the consultation itself is credited toward your first month’s membership when you commit to a 6- or 12-month program with us.”
It works for two reasons.
First, it rewards the longer commitment.
You are paying patients in their own already-spent money to lock in for 6 or 12 months.
That is exactly the behavior a recurring-revenue clinic wants.
Second, it gives the provider a generous-sounding reason to ask for the commitment on the call.
That is much better than letting the patient drift off to think about it.
One caution from the field: if patients tend to group the entry costs together, keep the framing as one $600 number credited toward the first month.
Do not itemize labs and consult separately if that makes the patient feel double-charged.
Why should you collect the credit card on the discovery call instead of sending a payment link?
Because the commitment is strongest at the moment the patient says yes.
Every minute between the verbal yes and the payment is a minute they can cool off, get distracted, or never open the link.
The most common way clinics lose a closed discovery call is by getting the verbal commitment and then sending a Zelle, Venmo, or card link to be paid later.
The patient says, “yes, I want to move forward.”
The provider books the labs.
Then the payment never comes through.
The link sat in a text thread while life happened.
The fix is to collect the card on the phone while the patient is still committed.
The moment they say they want to move forward, say:
“Great — let me grab a card to hold your spot.”
Then take the number right there.
Offering a no-fee option like Zelle or Venmo is fine.
But offer it as a choice after you have the commitment.
Do not send it as a link instead of asking.
If asking for the card feels pushy, remember that asking for payment after a yes is completely normal.
Get the commitment and the card on the same call.
Clinics that nail this see it compound at volume.
The same discipline that lets a practice like VYVE Wellness handle 100+ inbound calls a month only pays off when each one is closed and collected before the patient hangs up.
What exact words make membership pricing land on a discovery call?
Lead with “personalized” and “affordable.”
Frame the membership as the outcome of the consult.
Then offer two options so the patient chooses instead of deciding yes or no.
The two words that consistently move cash-pay patients are:
- Personalized
- Affordable
This line outperforms any version that opens with a price:
“From that consultation, we’ll put together a personalized, affordable membership program for you that makes sense.”
It sells the plan before the number.
The second move is to give options:
“We’ll present you two different options, and you can choose the one that makes the most sense to you.”
That shifts the patient’s brain from yes-or-no to which-one.
And a patient choosing between two plans is a patient who has already decided to join.
Build one lower-investment option and one fuller option.
That creates a real choice with a clear step up.
Then present them once you have earned the right to recommend a specific tier.
There is a harder truth underneath all of this from the field: the surest way to get a patient to actually engage with the plan is to charge them enough that it matters to them.
A program priced like it is valuable gets treated like it is valuable.
How do you transition existing patients to membership without forcing it on them?
Make membership the default for everyone moving forward while grandfathering past patients.
Then set the expectation through the website and the discovery call.
That way, the model feels like the natural way the practice works — not a new fee.
Many clinics want to move to a membership model but freeze because they do not want to alienate existing patients.
The clean answer is to draw a line.
Membership becomes the standard path for every new patient from this point on.
Patients who came before are left as they are unless they choose to upgrade.
That removes the fear of forcing anyone while still building the recurring base.
The key is setting the expectation everywhere a patient encounters you.
The website should say plainly that after the comprehensive consultation, you create a personalized, affordable plan.
It should also explain that there are membership programs to continue care.
The discovery call should echo the same message.
When a patient hears the same message on the site, on the call, and in the follow-up email, membership stops feeling like an add-on.
It starts feeling like simply how the practice works.
That consistency is what turns one-time consults into a recurring book of business.
FAQ’s About Discovery Calls and Membership Pricing
Should you mention membership pricing on the discovery call or save it for after the patient pays?
Mention it on the discovery call, but frame it as what happens after they get started.
Never frame it as a second price they have to weigh against the first.
Set the expectation that the entry fee gets them into the practice.
Then, from the consult, you build a personalized, affordable membership program to stay.
Save the actual dollar figures for after the consult, when you have a reason to recommend a specific tier.
How do you use the discovery call to anchor the membership price so it feels small?
Anchor against the $600 entry fee and the value of the personalized plan first.
That way, a $199 to $499 monthly membership reads as the affordable continuation rather than a new expense.
State the entry investment.
Describe the comprehensive panel and personalized protocol.
Then introduce the membership as the way to stay.
Adding a gift — crediting the consult cost toward the first month — makes the membership feel like something the patient gets rather than loses.
What is the credit-back framing and why does it convert discovery calls into members?
The credit-back framing credits the money the patient already spent on the consult toward their first month’s membership.
That happens when they commit to a 6- or 12-month program.
It works because it changes the emotional math.
The entry fee becomes a down payment they get back, rather than a second charge.
It also gives the provider a generous reason to ask for the commitment on the call.
Why should you collect the credit card on the discovery call instead of sending a payment link?
Because the commitment is strongest at the moment the patient says yes.
Every minute between the verbal yes and the payment is a minute they can cool off or never open the link.
Take the card on the phone the moment they say they want to move forward.
Offer a no-fee option like Zelle or Venmo as a choice after the commitment.
Do not use it as a link sent instead of asking.
What exact words make membership pricing land on a discovery call?
Lead with “personalized” and “affordable.”
Frame the membership as the outcome of the consult.
Then offer two options so the patient chooses instead of deciding yes or no.
“From that consultation, we’ll put together a personalized, affordable membership program for you that makes sense” sells the plan before the number.
“We’ll present you two different options” shifts the patient from yes-or-no to which-one.
How do you transition existing patients to membership without forcing it on them?
Make membership the default for every new patient moving forward while grandfathering past patients.
Then set the expectation through the website, the discovery call, and the follow-up email.
That way, the model feels like simply how the practice works.
Drawing that line removes the fear of forcing anyone while still building the recurring base.