How Should a Cash-Pay Regenerative or Pain Medicine Clinic Layer a Hormone Membership for Recurring Revenue?
The regenerative or pain clinic that adds a properly-structured hormone membership picks up $100K–$300K+ in additional annual recurring revenue from the patients it’s already treating. Get the pricing, medication transaction ownership, and billing cadence right and the membership compounds. Get any one of them wrong and the patient quits before month three.
A cash-pay regenerative or pain medicine clinic — stem cells, PRP, peptides, prolozone, shockwave — is one of the highest-trust environments in healthcare. Patients who pay $8K for stem cells will pay $300–$400/month for hormones and labs from the same provider, if the membership is structured correctly. Below is the model we recommend on weekly strategy calls with regenerative and pain clinics that are layering in hormones for the first time, the specific pricing math, the billing cadence that retains, and how Direct Primary Care can sit inside the same membership to double the LTV.
Why should a cash-pay regenerative or pain medicine clinic layer a hormone membership on top of stem cell/PRP/peptide treatments?
Because regenerative and pain patients are:
- already paying cash
- already trust the provider
- almost universally have at least one hormonal imbalance contributing to whatever they came in for
Examples:
- low T contributing to joint deterioration in men
- hormonal shifts contributing to soft-tissue inflammation in women
- cortisol issues contributing to slow recovery in athletes
The same patient who paid:
- $6,500 for stem cells in their knee
…will pay:
- $400/month for hormones and labs
…from the provider they already trust — but only if:
- you actually offer it
- you offer it in a structure that makes the membership feel like ongoing care, not an upsell
Add the math:
A regenerative practice with:
- 25–40 active members on hormones
…is producing:
- $100K–$200K/year in recurring membership revenue
…on patients it’s already acquired, with almost zero marginal acquisition cost.
Many regenerative providers discover that layering a hormone membership onto a pain clinic is one of the fastest ways to create predictable recurring revenue from an existing patient base. Rather than relying entirely on episodic procedures, clinics can build a membership model that compounds patient lifetime value while strengthening long-term outcomes.
That cushion is what lets regenerative clinics:
- survive a slow month on the stem cell or PRP side without panicking
The membership is:
- the keel
What’s the $300/$300/$300 pricing model — and why does it convert better than legacy $6K–$8K hormone programs?
The model is:
- $300 for labs
- $300 for the initial consult
- $300/month for the membership
…with the consult fee credited toward the first month so the patient feels they:
- “got the consult free”
The membership includes:
- all follow-up labs
- all follow-up consults
- the cost of medications
- a 15%-off-everything discount on:
- peptides
- weight loss meds
- supplements
- aesthetic services like Botox
Legacy:
- $6K–$8K one-time hormone programs
…that were standard 5–10 years ago have largely stopped selling.
Patients now expect:
- a subscription model
…that mirrors:
- their gym
- their streaming services
- their telehealth
A New York clinic that sold:
- $6K–$8K programs for a decade
…now sells the same care at:
- $650 initial consult
- $450/month
…and is growing again.
The pricing also gives you room to grow.
A clinic outside Sacramento:
- started at $300/month
- raised to $350/month a year in
- raised again to $400/month five months ago
…all because demand kept supporting the increases.
They sit at roughly:
- 320 active members
…which is about:
- $1.5M/year in pure membership revenue
The clinic that anchors its pricing at:
- $300/month
…and never raises is leaving:
- 30–40% of mature-market revenue on the table
Why does owning the medication transaction matter for hormone membership retention?
Because when the patient picks up their hormones at an outside retail pharmacy:
- they mentally separate the prescription from the membership fee
…and the monthly charge starts to:
- feel optional
When the clinic owns the medication transaction:
- the compounding pharmacy bills the clinic
- the clinic ships directly to the patient or stocks in-house
…the patient experiences the membership as:
- ongoing comprehensive care
…not:
- a recurring lab fee
The medication and the membership are:
- linked in their mind
That linkage is one of the single biggest separators between:
- hormone membership programs that retain at 80%+ year-over-year
- programs that lose 40% of patients in the first six months
Set the relationship up with the compounding pharmacy on day one.
- They bill you
- you bill the patient through the membership
- the patient never has to think about:
- which pharmacy
- which copay
- which fill date
The administrative overhead is:
- real but small
…and it is what makes the membership feel like membership instead of:
- a recurring lab subscription

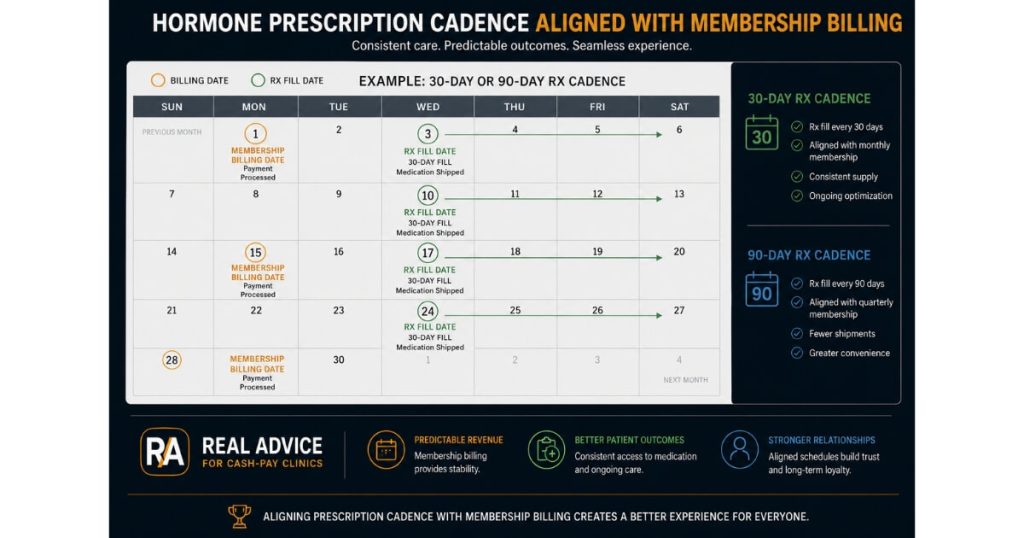
Should hormone membership billing match the prescription supply cycle?
Yes — misaligned cadence is one of the top reasons patients quit a hormone membership even when they like the clinical results.
If you:
- dispense a 90-day supply of testosterone, peptides, or whatever the patient is on
- but charge the patient monthly
…the transaction stops lining up with the value they’re physically holding in months two and three.
They feel:
- billed for nothing
Solve this in one of two ways:
- bill the membership quarterly to match a 90-day fill
- break the prescription into 30-day fills so each charge corresponds to a visible delivery
The 30-day-fill version is:
- psychologically stronger
…because each month brings:
- a new tangible package
The quarterly version is:
- operationally simpler
Either is dramatically better than:
- 30-day billing on a 90-day supply
…which is:
- the default
- the silent killer of hormone memberships
The HRT clinic we scaled from $1M to $4M/year runs on:
- 30-day fills aligned to 30-day billing
…the cadence makes the membership feel:
- inevitable
Should I lead new hormone patients with pellets, or with injectables and creams?
For new hormone patients — especially patients who have never been on TRT or HRT before — lead with:
- injectables
- creams
- patches
…because the perceived risk is:
- reversible
The patient can:
- try the protocol for 6–8 weeks
- stop if they don’t feel right
Pellets:
- feel scary to a hormone-naive patient
…and a meaningful percentage of patients who had:
- a bad pellet experience years ago
…refuse to repeat it.
You don’t want to lose the consult over:
- a modality decision
Keep pellets on the menu though.
A segment of experienced hormone patients:
- won’t book unless pellets are offered
Offer both:
- let the patient self-select after a month or two on the lower-risk option
Many will:
- progress to pellets once they trust the clinic
The decision tree:
- new patient
→ injectable/cream
→ 60-day reassessment
→ pellets if the patient wants the convenience
→ continue injectable if not
Should I bundle Direct Primary Care into the hormone membership — and what does the math look like?
Yes, bundle DPC inside an upgraded:
- $350–$450/month tier
…especially if local insurance-based practices are making patients:
- wait three weeks for an appointment
A two-physician ER group outside Santa Rosa Beach, Florida:
- built DPC to $60,000/month at $275/month in eighteen months
A New York clinic:
- now includes DPC inside a $450/month hormone membership
- is closing it as a single unit
The bundle works because the patient gets:
- convenience
- same-day access
- direct phone line to the provider
- no insurance friction
…at a lower price than the hormone membership alone would deliver elsewhere.
The math at the clinic level is straightforward.
Start the bundle at:
- $350/month
…while it’s:
- a no-brainer
- under-priced relative to value
Then:
- build a base of 25–50 patients
- raise prices as demand confirms
At:
- 100 bundled members
…you’re producing:
- $35K–$45K/month in recurring revenue
…from patients who are also paying for:
- regenerative procedures
- aesthetic procedures
…throughout the year.
The clinics that win this play are the ones that move while local insurance-based practices are making patients wait — which, in most US metros in 2026, is right now.
How many DPC patients can one provider realistically panel — and what does that mean for staffing?
Plan for roughly:
- 250 DPC patients per provider
…with normal support staff to handle:
- phones
- scheduling
- lab draws
A seasoned provider with strong systems can push toward:
- 450 patients
…but only with:
- operations help
- a tightly run intake
Most clinics in our portfolio that have layered DPC successfully sit between:
- 200–350 patients per provider
…well below theoretical capacity.
Which means:
- there is room to grow into the panel before adding a second provider
The implication for staffing:
You don’t need to hire another physician to break:
- $500K/year in DPC revenue
…at a single-provider clinic.
You need:
- a clinical assistant or NP who handles routine touchpoints
- a front desk who triages every inbound call inside 5 minutes
- a CRM that surfaces who hasn’t been seen in 60–90 days
Hire support before you hire another provider.
The math almost always favors:
- deeper utilization of the provider you already have
…before:
- adding capacity
The pain management practice we added $2.095M in revenue to in 10 months did it with:
- disciplined panel utilization
- inbound conversion
…not by aggressively hiring providers.