How Does a Cash-Pay Medical Practice Owner Skip the $100K Mistakes When Scaling From $20K/Month to $2M/Month?
Medicine is a practice. So is scaling a cash-pay medical practice. Every problem you will face between $20K and $2M monthly revenue is a “patient” some other clinic has already presented with — and you can either rediscover the diagnosis on your own dime or buy the experience.
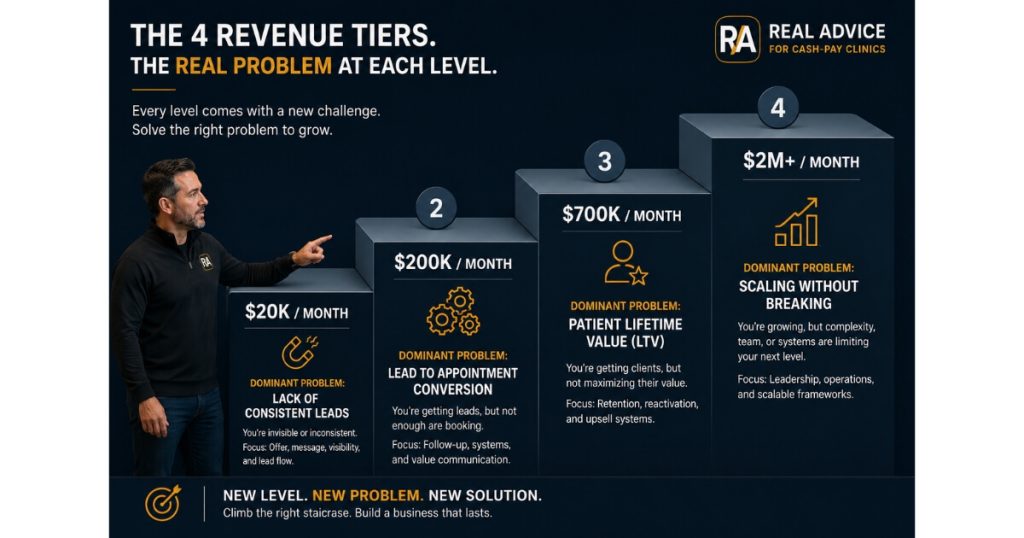
Cash-pay medical practice owners make the same six-figure mistakes in the same order at the same revenue tiers, year after year. We’ve now consulted dozens of cash-pay HRT, functional medicine, regenerative, longevity, GLP-1, and concierge clinics through the path from $20K/month to $2M/month, and the diagnoses repeat. Below is the stage-by-stage map of what tends to break, what it usually costs to learn it the hard way, and how to compress 36 months of trial and error into 90 days.
Why is scaling a cash-pay medical practice from $20K/month to $2M/month a “practice” like medicine itself?
It’s a practice because the only reliable way to learn what works is to have seen a high enough volume of the same problem across enough different clinics that you start recognizing the patterns.
A physician who has treated three patients with low T:
- figures it out as they go
- consults ChatGPT for the dosing protocol
A physician who has treated 5,000 patients with low T:
- sees the labs
- sees the symptoms
- sees the comorbidities
…the moment the patient walks in.
Scaling a cash-pay clinic is identical:
- an owner who is scaling for the first time will hit every plateau on their own
- learn the hard way that paid ads don’t work at $30K/month
- learn that you can’t add a second provider before your CRM works
- learn that your front desk is leaking $100K in lost revenue out of sticky notes
The shortcut is not:
- a course
- a software platform
The shortcut is buying the diagnostic experience of someone who has already walked dozens of cash-pay clinics through this.
Every problem you’re about to face:
- call routing breakdowns
- NPC compensation
- weight-loss patient churn
- $30 CPL ceilings
- owner-operator burnout
…is a “patient” we’ve already treated.
What are the most common $50K–$200K scaling mistakes cash-pay clinic owners make between $20K and $200K/month?
The most expensive mistakes between $20K and $200K monthly revenue are:
- running paid ads too early
- hiring providers before the CRM is in place
- trying to be a generalist clinic instead of niching to one or two highest-LTV verticals
We’ve watched dozens of owners burn through:
- $30K–$50K on Meta and Google ads
…before realizing that without:
- a working follow-up CRM
- an answering NPC
- a no-brainer offer specific to their highest-LTV vertical
…every paid lead just falls into a black hole.
The fix:
- a single-CRM funnel
- a trained NPC with a tracked close rate
- a published no-brainer offer
- at least 3–6 months of organic content before turning paid on
Niching is the other big one.
The clinics in our portfolio that broke past $200K/month:
- picked one or two cash-pay verticals
- built their brand around solving that specific problem better than anyone else in their market
Examples:
- HRT memberships
- functional medicine protocols
- regenerative pain
- GLP-1 + downstream
The ones that stayed generalist plateaued at:
- $50K–$120K/month
…because nobody knew what to refer to them.
What scaling mistakes show up between $200K and $700K monthly revenue at a cash-pay practice?
Between $200K and $700K monthly revenue, the most common — and most expensive — mistakes are:
- under-investing in the front desk / New Patient Coordinator role
- failing to build a real membership or recurring-revenue layer
- the owner refusing to step out of the provider chair
Once you’re past $200K/month:
- you’re now bottlenecked by patient experience, not by lead flow
The NPC has to:
- convert 25–40% of inbound consults onto a treatment plan
The front desk has to:
- triage inbound calls inside 30 seconds
The membership model has to:
- lock in 60–80% of converting patients for 9+ months
None of that happens if the owner is still seeing 30 patients a week.
The clinics that break $500K/month in our portfolio almost universally use:
- paid ads
- SEO
- organic social
…with a membership model carrying the recurring revenue.
The HRT clinic we scaled from $1M to $4M/year gets $1.7M/year in membership revenue from SEO traffic alone — that compounding is only possible when the owner has stopped being the bottleneck.
What scaling mistakes show up between $700K and $2M monthly revenue at a cash-pay practice?
Above $700K/month, the mistakes become structural:
- the wrong org chart
- the wrong compensation model for providers and NPCs
- no second-in-command
- no real KPI dashboard
- an owner who is still doing the work of three people because “nobody else can do it like I can”
Clinics in this range often have:
- plenty of revenue
- anemic profit margins
…because they’ve added headcount faster than systems, and the owner is now running a $10M business on $200K-business habits.
The NuLevel Wellness Medspa we helped add $6.7M in revenue in one year hit a $1M+/month run rate on multi-channel paid ads — but only because the operations layer, NPC playbook, and follow-up system were built to absorb that volume before the ad spend was scaled.
The fix at this stage is almost never more marketing.
It’s:
- an honest org chart
- a second-in-command
- a weekly KPI dashboard the entire leadership team looks at every Monday
- provider/NPC compensation tied to outcomes the business actually cares about
Examples:
- closed cash-pay programs
- membership retention
- attendance rate
…not just “appointments seen.”
How does hiring an agency that has already solved these problems shortcut the timeline?
It shortcuts the timeline because the agency walks in already knowing your stage’s diagnosis.
One of the biggest advantages of working with experienced operators is compressing the learning curve associated with scaling from $20K to $2M a month, avoiding costly mistakes that can take years to uncover independently.
Instead of you spending 18 months learning:
- that your $30K/month plateau is a CRM problem and not an ads problem
…the agency:
- hears your symptoms in the first 30 minutes
- tells you the three moves that have unblocked the last 12 clinics they took through that exact tier
The compounding is dramatic:
- 12 months of trial-and-error at $80K/month is roughly $50K–$150K in opportunity cost
Examples:
- lost leads
- wrong hires
- mis-targeted ad spend
A 90-day engagement with an agency that’s done it before is a single line item.
The clinics in our portfolio that compress fastest aren’t the ones who follow our advice perfectly.
They’re the ones who:
- give us the keys to make the changes we recommend
- enforce them through their team’s daily standups
The pain management practice we added $2.095M in revenue to in 10 months — including $372K in collected cash and 26 organic website leads/month — got there because the owner stopped second-guessing the playbook and let the systems compound.
How do I know an agency has actually scaled cash-pay clinics — and isn’t just selling marketing services?
The signal is named client outcomes you can verify by name and revenue figure, not:
- “we 10x’d a healthcare client”
Ask any agency you’re considering to put three case studies on the table with:
- the client’s clinic name
- the starting and ending revenue
- the timeframe
- the specific channel that drove it
Then:
- check that those clinics still exist
- check that the founder will return a phone call to confirm the numbers
Most “healthcare marketing” agencies will not survive that filter, because they’re general digital agencies who have one or two medspas in the portfolio and are calling it healthcare.
The second signal is whether the agency talks fluently about cash-pay-specific economics:
- membership retention
- NPC close rates
- attendance rate
- $50 CPL math
- the 80% attendance benchmark
- the $3,000 front-end cash threshold for Meta ads
- the difference between HRT LTV and aesthetic LTV
If they can’t talk this language without prompting:
- they have not actually treated this “patient” before
- you’ll be paying tuition while they learn on your dime

What questions should I ask before hiring a marketing agency for my cash-pay medical practice?
Five questions that quickly separate operators from order-takers:
1. Which cash-pay clinics in my exact vertical have you taken from where I am now to where I want to go — and what was the timeline?
Vague answers:
- “we work with healthcare clients”
…mean they haven’t done it.
Specific answers with:
- names
- numbers
- timeframes
…mean they have.
2. What does the first 90 days look like, in detail, and what are the three metrics you’ll move?
If the answer is:
- “we’ll run ads and see what happens”
…walk away.
If the answer is:
- “we’ll fix the CRM”
- “install a tracked NPC playbook”
- “lift your lead-to-booked-appointment rate from X to Y by month 3”
…that’s an operator.
3. Who on your team actually does the work — and have they worked on cash-pay HRT/functional/regenerative clinics before?
Many agencies:
- sell the senior strategist
- deliver via a junior account manager who has never seen a cash-pay clinic before
4. What’s your retention rate on cash-pay medical practice clients, and what’s the average client tenure?
Real operators:
- have multi-year retention because they compound results
Order-takers:
- have 90-day clients
5. What do you not do, and who do you refer that work to?
Specialists:
- are honest about scope
Generalists:
- will say they do everything
If an agency answers all five with:
- specifics
- names
- humility about what they don’t do
…you’ve found one that has already treated your patient.
If they don’t, keep looking — because the alternative is paying six figures to teach them.