Why Should I Start With My Message Before Choosing a Marketing Channel for My Cash-Pay Medical Practice?
The most expensive marketing mistake we see at cash-pay clinics is picking the channel first — “Dr. Smith said he gets all his business from Facebook, so let’s run Facebook ads” — and then trying to retrofit a message and market to the channel. It usually costs $30K–$50K in wasted ad spend before the owner figures out the channel wasn’t the problem. Here’s the order that prevents the loss.
The Message-Market-Media framework says you build a marketing campaign in that order — Message first, Market second, Media last. Most cash-pay clinic owners do it exactly backwards: they hear another doctor talking about Facebook, TikTok, Google Local Services Ads, or whatever the channel-of-the-month is, and they start there. Below is why the order matters, how to actually define each component, and the channel-to-specialty cheat sheet we’ve built across more than a decade of running campaigns for cash-pay HRT, functional medicine, regenerative, longevity, weight loss, ED, and aesthetic practices.
What is the Message-Market-Media framework — and why does the order matter for a cash-pay clinic?
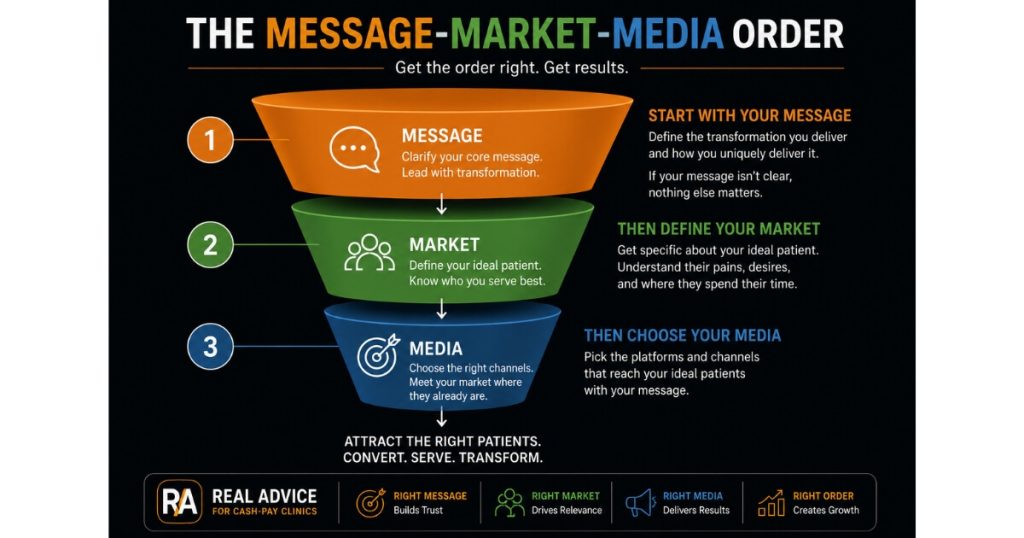
The framework says every campaign has three components:
- your Message (the result you produce for patients)
- your Market (who you produce that result best for)
- your Media (the channel you reach them on)
The order matters because:
- a wrong-order campaign costs five-figure sums to discover what was actually broken
When you pick the Media first:
- “I want to run Facebook ads”
…you have no anchor to evaluate whether the ads underperformed because of:
- the channel
- the targeting
- the offer
- the creative
- the patient avatar
…and your team will spend:
- 90 days iterating on the wrong thing
When you build:
- Message
- Market
- Media
…in order, every downstream decision is constrained by an upstream truth.
The flow:
- The Message tells you who responds to it (your Market)
- The Market tells you where they hang out and how they research (your Media)
By the time you’re picking the channel:
- the channel is almost obvious
…and the testing budget you save is:
- the budget that funds the next 90 days of campaigns
How do I write my Message before choosing my Market or Media?
Your Message is:
- the specific result you produce
…written in:
- one short sentence
- plain English
Example of a Message:
“I help cash-pay medical practices build, grow, and scale patient acquisition systems”
Example of what is NOT a Message:
“I do marketing for doctors”
That’s:
- a category
- not a result
A Message for an HRT clinic might be:
“I help men 38–55 get their energy, libido, and edge back through optimized hormone therapy and lab-led membership care.”
A Message for a regenerative pain clinic might be:
“I help active 45–65-year-olds avoid surgery and get back to the sports they love through stem cells, PRP, and shockwave.”
The test of a strong Message:
The person reading it can immediately tell whether:
- they are the right patient
If they can’t:
- the Message is too generic
Rewrite it until:
- the wrong patient self-deselects in the first 10 seconds
The clinics in our portfolio that rewrote their Message before re-running ads consistently saw CPL drop and close rates climb. The reason is simple: starting with message before channel creates stronger alignment between patient needs, marketing strategy, and media selection.
How do I define my Market once my Message is clear?
The Market is:
- the specific patient who responds best to your Message
…defined by:
- demographics
- psychographics
- behaviors
Example:
“Cash-pay HRT for men 38–55, household income $150K+, who have already tried optimization on their own (gym, supplements, sleep tracking) and have hit a wall they suspect is hormonal”
NOT:
“Anyone with low testosterone”
That’s:
- a symptom
- not a patient
Narrow the Market enough that:
- you can name three current patients who fit it perfectly
If you can’t:
- your Market definition is still too broad
The Market definition also tells you:
- what the patient already believes
- what they’ve already tried
- what they’re skeptical of
…which becomes the raw material for:
- your messaging
- your landing pages
- your NPC consult script
The HRT clinic we scaled from $1M to $4M/year defined a Market so specific that:
- the marketing copy
- the consult script
- the membership offer
…all converged into:
- a single voice
…and the compounding showed up across:
- every metric
Why is choosing the Media (channel) last actually the right move?
Because:
- Media is a derived decision
- not an opening decision
Once you know:
- your Message (the result)
- your Market (the patient)
…the question of:
- where to find that patient
…almost answers itself.
Examples:
- A 50-year-old male professional researching low T is on YouTube and Google, not TikTok
- A 32-year-old woman researching non-surgical aesthetics is on TikTok and Instagram, not LinkedIn
- A 60-year-old with chronic knee pain considering an alternative to surgery is on Google with high commercial intent, not on Facebook scrolling for entertainment
Picking Media last also lets you:
- sequence channels by intent
High-intent search channels:
- Google Search
- Google LSA
- YouTube education
These:
- tend to convert fastest
- cost more per click
Lower-intent social channels:
- TikTok
These:
- tend to be cheaper per click
- require more nurture before conversion
With Message and Market locked in, you can sequence:
- start with the highest-intent channel for your specialty
- prove the unit economics
- layer in cheaper-but-slower channels as you scale
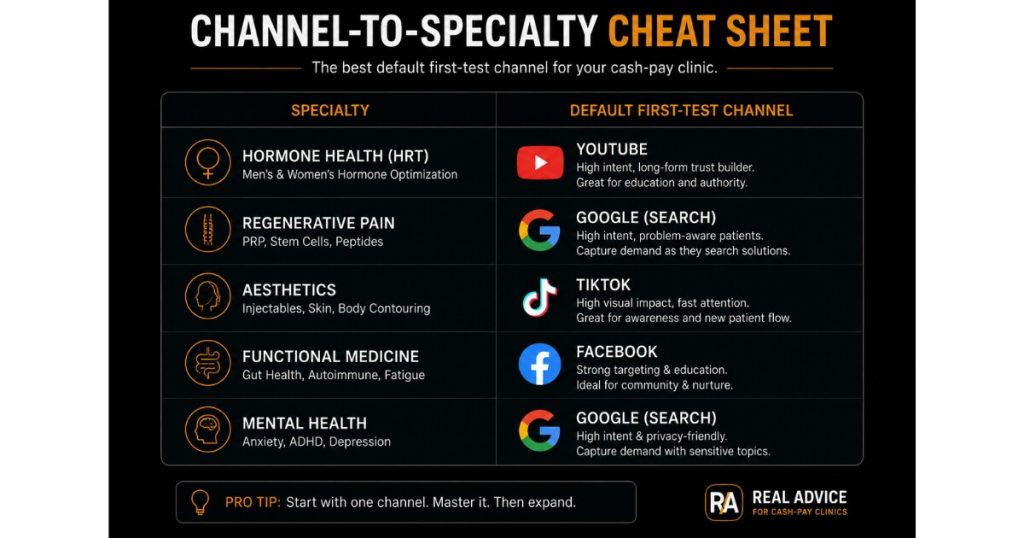
What’s the single channel I should test first for each cash-pay specialty (HRT, weight loss, pain, ED, aesthetics)?
After 12+ years of running campaigns for cash-pay clinics, these are the default first-test channels we’d recommend by specialty.
HRT / TRT / peptides:
- YouTube
The demographic is:
- researchers
…and YouTube is where they live before Google.
Use:
- VidIQ or similar for keyword research
Build content around:
- symptoms first
- “Why does my energy crash at 2 PM?”
- modality second
Pain / regenerative (knees, shoulders, hips, back, spine):
- Google Search
Why:
- Highest intent
- Fastest-converting leads
- Most expensive per click
…because you’re competing with:
- insurance
- law firms
- other pain clinics
Edit your landing page to avoid keywords like:
- “stem cell”
…that Google will reject.
Expect:
- ~50% conversion from Google leads
- ~15–20% from Facebook leads
Erectile dysfunction:
Why:
- Men want a solution
- they don’t shop
- they convert fast
…but you’re competing against:
- Hims
- Roman
…so expect:
- higher CPCs
GLP-1 / semaglutide / tirzepatide:
- Google if you have LegitScript approval
- YouTube if not
The intent is:
- high
The offer has to be:
- precise
Aesthetics:
- Instagram or TikTok
Why:
- Your market is women comparing themselves to other women
- that’s where they spend time
Use:
- a discount offer
- “$150 off non-surgical facelift”
Have the front desk ready to:
- call within minutes of the lead form
These patients:
- move fast
- are loyal once converted
Why has Facebook stopped being the default channel for cash-pay clinics — and when does it still work?
Facebook hasn’t stopped working, but:
- it has stopped being the default
Why:
- lead quality has deteriorated
- the operations required to convert Facebook leads have intensified
Example:
A Facebook lead in 2018:
- could be called once and booked
A Facebook lead in 2026:
- typically needs to be called within 5 minutes
- then called 2–3 more times the same day
- then nurtured through a CRM sequence for 7–14 days before they convert
That requires:
- a trained NPC
- a tight CRM
- the bandwidth to call leads at 8 PM on a Tuesday
Most cash-pay clinics under:
- $100K/month
…don’t have that operational stack.
Where Facebook still works:
- clinics with a large team of patient care coordinators or receptionists
- clinics with high-ticket programs that justify intensive nurture
- pain clinics
- surgery clinics
- longevity programs above $5K
- aesthetics
- GLP-1 weight loss for patients who aren’t yet committed to a specific protocol
Facebook can absolutely scale.
The medspa we helped add $6.7M in revenue in one year used Facebook as:
- a major channel
…but only because:
- the operational layer underneath it was built to absorb the volume
What are the common Message-Market-Media mismatches that waste cash-pay marketing dollars?
Three mismatches show up over and over.
Mismatch 1: Message-Media gap
The clinic has:
- a sophisticated, niched Message
- “longevity care for high-performing executives”
…but runs it on:
- TikTok
…where the average watcher isn’t:
- a high-performing executive
The Message is fine.
The Media is wrong.
Move the same content to:
- YouTube education
- a podcast sponsorship
…and the Message lands.
Mismatch 2: Market-Media gap
The clinic has:
- a clear Market
- women 45–60 with perimenopausal symptoms
…but runs Google Search ads aimed at:
- men 25–35
…because that’s who searches:
- “low T near me”
The Market is fine.
The Media targeting is wrong.
Either:
- retarget the Google campaign
- move to YouTube
…where women 45–60 are actively researching:
- menopause
- HRT content
Mismatch 3: Message-Market gap
The clinic has:
- a strong Media presence
- a good Instagram account
- a working Google campaign
…but the Message is generic:
- “we help you feel better”
…so the Market is:
- everyone
…which is:
- no one
Rewrite the Message until:
- the wrong patient self-deselects
…and CPL drops without changing:
- a single channel
Fix the mismatch farthest upstream first.
The downstream metrics:
- correct themselves