What Does a 10:1 Return on Ad Spend Actually Take at a Cash-Pay Medical Practice? ($2,700 In, $25,000 Out)
A cash-pay clinic spent $2,700 on ads last month and pulled in about twenty-five thousand dollars. That is roughly ten dollars back for every dollar in — and it was not luck.
It was the boring stuff done right: a cost per booked call under a hundred bucks, calls that actually showed up, and an offer good enough that the people who showed actually bought.
Here is the FAQ on what a 10:1 return on ad spend actually takes at a cash-pay medical practice — and why the ad almost never deserves the credit or the blame.
What does a 10:1 return on ad spend actually look like at a cash-pay medical practice?
About $10 back for every $1 spent — $2,700 in ad spend producing roughly $25,000 in revenue inside a single month.
That is the headline number, but the headline is the least useful part.
A 10:1 month is not a clever creative or a secret targeting trick.
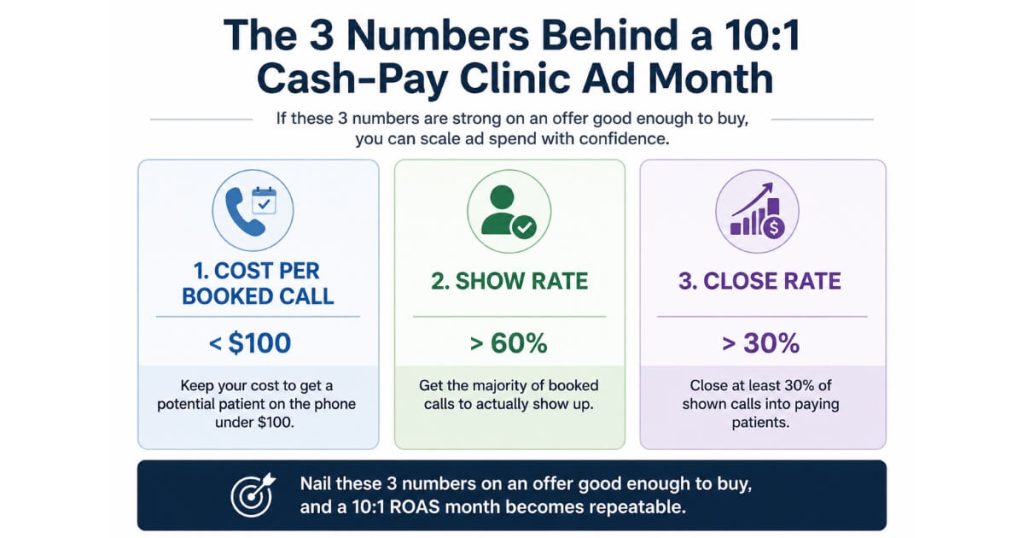
It is three boring numbers stacked on top of each other:
- Cost to book a call
- Share of booked calls that actually show
- Share of show-ups that buy
When all three are healthy at the same time, the return looks spectacular.
When any one of them is broken, the same ad budget looks like a waste.
The clinics that hit these returns are not running fundamentally different ads than everyone else.
They are running the same ads into a far better machine — and the machine is what produces the multiple.
Why do ads “expose” your offer instead of fixing it?
Because ads do not create demand for a bad offer — they just buy you more chances to fail at converting it.
Here is the truth most clinic owners learn the expensive way:
Ads do not fix a broken offer.
They expose it.
If your offer is weak, your intake is sloppy, or your follow-up is slow, more ad spend simply produces more leads who slip through the same cracks — faster, and at a higher cost.
The platform did its job.
It delivered humans who raised their hand.
Everything that happened after the click is on the practice.
This is why two clinics in the same city, selling the same treatment, running nearly identical ads, get wildly different results.
One is spending $2,700 to make $25,000.
The other is spending $2,700 to make $4,000 and blaming the ad account.
The difference is never the ad.
It is the offer the click lands on and the intake process that catches it.
What’s a good cost per booked call for a cash-pay medical practice?
Under $100 per booked call is the benchmark that makes the rest of the math work at most cash-pay clinics.
In the 10:1 month, cost per booked call came in under a hundred dollars.
That number matters more than cost per lead because:
- A lead is just an email address.
- A booked call is a human who picked a time.
If you are paying under $100 to put a qualified, scheduled call on the calendar, and your offer is strong enough to carry the conversation from there, the economics almost always work.
But the benchmark only means something when paired with the next two numbers.
- A $40 booked call is worthless if nobody shows.
- A 90% show rate is worthless if the offer does not close.
Cost per booked call is the entry ticket.
Show rate and close rate are what turn the ticket into revenue.
Why do show rate and close rate matter more than the ad itself?
Because the ad’s only job is to produce a booked call — everything that determines whether that call becomes money happens after the click.
A booked call that no-shows cost you the full acquisition price and returned nothing.
A booked call that shows but does not buy means the offer was not good enough for the person who was interested enough to sit down.
In the 10:1 month, the calls showed up and the show-ups bought — not because of the ad, but because the offer was compelling and the intake was tight enough to keep the appointment warm between the click and the call.
This is the part clinics underinvest in.
They will spend weeks A/B testing ad headlines and zero hours fixing the reason 40% of their booked calls ghost.
The leverage is backwards.
We watched a multi-channel paid program compound exactly this way at a weight-loss and medspa clinic where we added $6.7M in revenue in one year across 3,727 new patients:
The ads scaled only because the offer and the follow-up behind them could absorb the volume without leaking it.
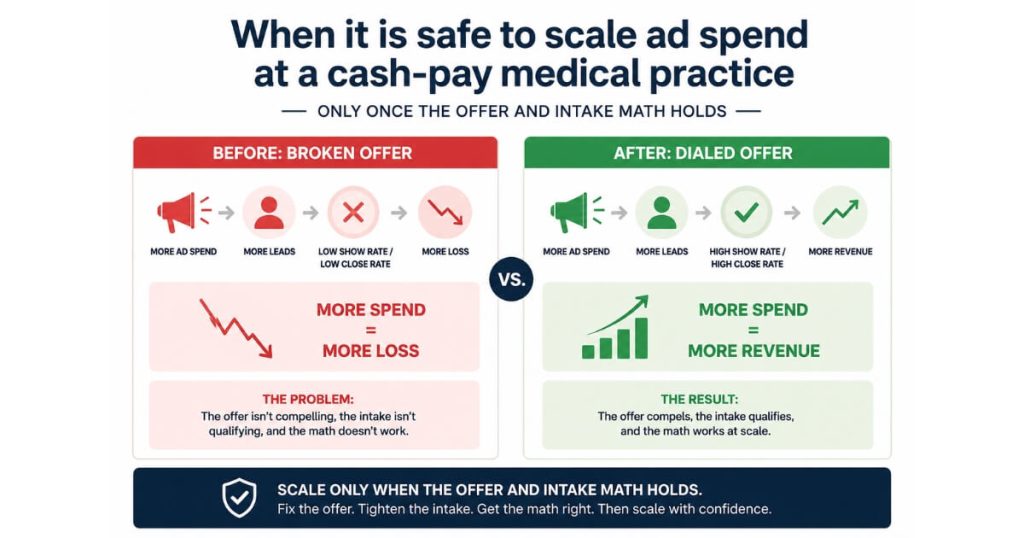
When is it safe to scale ad spend at a cash-pay medical practice?
The moment the math holds — when you know that another dollar in reliably produces several dollars out.
Scaling is scary for most owners because they have never proven the unit economics.
They do not actually know:
- What a booked call costs
- What their show rate is
- What their close rate is
So “spend more” feels like “gamble more.”
But when those three numbers are dialed in and stable, spending more stops being a gamble and becomes arithmetic.
You are not hoping for a good month.
You are buying a known return at a known multiple.
That is the real definition of “ready to scale”:
Not a revenue threshold.
Not a number of months in business.
A proven, repeatable conversion machine where adding spend predictably adds revenue.
Until you have that, more budget just amplifies whatever is already broken.
If my ads aren’t returning multiples, what’s actually broken?
Almost always, it is everything that happens after the click — not the ad itself.
Run the diagnosis in order.
1. Cost per booked call
If it is wildly high, the offer in the ad is not compelling enough for people to schedule.
2. Show rate
If booked calls are not showing, the gap between booking and the appointment is too long or too cold.
There is no confirmation sequence.
There is no reminder.
There is no reason to show.
3. Close rate
If show-ups are not buying, the offer itself is not strong enough or the person taking the call cannot carry it.
Notice that none of those three fixes is “make a better ad.”
If your ads are not coming back in multiples, the problem is usually not the ad.
It is the offer it lands on and the intake that catches it.
Fix that, and the same ad budget you already have starts producing a different number.
That is exactly how dialed-in paid social produced $2 million in revenue from Facebook ads alone at an orthopedic surgical practice:
The offer, the ad team, and the follow-up were all in place at the same time.
FAQ’s About a 10:1 Return on Ad Spend at a Cash-Pay Clinic
How much revenue can a small ad budget produce at a cash-pay clinic?
A well-built cash-pay clinic produced about $25,000 in one month on $2,700 of ad spend — roughly a 10:1 return.
The budget size is not what drove it.
The offer, the under-$100 cost per booked call, the show rate, and the close rate did.
A small budget into a dialed-in machine beats a large budget into a leaky one.
Is a 10:1 return on ad spend normal for a cash-pay medical practice?
It is achievable but not automatic.
A 10:1 month happens when cost per booked call, show rate, and close rate are all healthy at once.
Many clinics never see it because one of those three is broken — and they blame the ad account instead of the offer and intake behind it.
Should I fix my offer or my ads first?
Fix the offer and the intake first.
Ads expose a weak offer.
They do not fix it.
Spending more on ads before the offer and follow-up are dialed in just produces more expensive leads that slip through the same cracks.
How do I know I’m ready to spend more on ads?
You are ready when the unit economics are proven and stable:
- A known cost per booked call
- A known show rate
- A known close rate
At that point scaling is arithmetic, not a gamble.
Another dollar in reliably returns several dollars out.
What’s more important, cost per lead or cost per booked call?
Cost per booked call.
A lead is an email address.
A booked call is a scheduled human.
Under $100 per booked call is the benchmark that makes the rest of the cash-pay ad math work — but only when paired with a strong show rate and close rate.
What’s the next step?
If you are running ads at a cash-pay medical practice and the returns are not coming back in multiples, the fix is almost never a new ad.
It is:
- The offer the click lands on
- The intake that catches the lead
- The follow-up that keeps a booked call warm until it shows
Get those three right and your existing budget starts producing a different number — the same way $2,700 turned into $25,000.
If your cash-pay practice is spending on ads and you want someone to pull apart your offer, your cost per booked call, your show rate, and your close rate — and tell you exactly which one is leaking — that is the conversation to book.
We will map the full path from click to cash on the call.