How Should a Cash-Pay HRT or Functional Medicine Clinic Build Its Patient Follow-Up and Retention System? (Filipino VA + GHL + Provider Note Discipline)
A cash-pay HRT or functional medicine clinic loses more revenue between visits than during them. A patient seen in September with a “follow-up in 4 weeks, blood draw in 3 weeks” instruction in the note quietly drifts past both of those windows, no one on the team is sure whether anyone reached out, and a paying, engaged patient stalls. Multiply that by a hundred patients across a growing practice and the leak becomes the largest unaddressed line item on the P&L. Here’s the FAQ on the follow-up and retention system that actually catches every patient — without hiring another full-time U.S. front desk.
Why do paying patients fall through the cracks at a cash-pay HRT or functional medicine clinic?
Because the next appointment didn’t get booked at the end of the current one — and once a patient walks out without a future appointment on the books, every follow-up becomes manual recovery work that gets crowded out by whatever’s louder that day.
The pattern looks identical across cash-pay clinics. A “good patient” — engaged, paying, on protocol — has a telehealth visit on September 2. The provider’s note says med pickup, follow-up in 4 weeks, blood draw in 3 weeks. A month later, nothing has happened. No one on the team is certain whether the patient was contacted, whether they ignored outreach, or whether they were never reached out to at all. The patient is “not a bad patient” — they were in clinic in July and August, they spend money — but they’re now two weeks past every instruction in their plan, and the clinic doesn’t know it.
The structural fix is to make booking the next appointment the default at the end of every visit. If the patient walks out (or hangs up the telehealth call) with the next date already on the books, the system has done its job. Everything else — automation, VAs, GHL workflows — exists to catch the patients who, for whatever reason, didn’t get booked at the visit. Treat the in-visit booking as the primary defense and the follow-up system as the safety net, not the other way around.
Who should own patient follow-up in a growing cash-pay clinic — the front desk, an MA, or a dedicated role?
A dedicated role. Patient retention is “$40-an-hour work” and gets crowded out the moment the front desk gets busy — and pulling a senior operator back into it is a trap because patients then only want to talk to that person and the role doesn’t scale.
The rule Anton uses across cash-pay clinics is:
“Give $40-an-hour work to $40-an-hour people and $20-an-hour work to $20-an-hour people.”
Front desk reception is $20-an-hour work — it’s interruption-driven, multi-tasked, and trains the staffer to triage rather than nurture.
Patient follow-up is $40-an-hour work — it requires:
- Reading the provider’s note
- Holding the patient’s plan in context
- Reaching out in a way that feels personal
When the two get bundled into one role, the $20 work crowds out the $40 work every single day, and the clinic only finds out when retention numbers slip a quarter later.
The cash-pay benchmark Anton points to is Eternity Health Partners (Santa Barbara):
- 250 active members
- Roughly 300 a la carte patients
- Dedicated client service coordinator at $80,000/year full-time
Separate from:
- Office manager
- Patient care coordinator
- Biller
- Phlebotomy / MA
The retention coordinator is the single highest-leverage hire in the practice and gets protected from front-desk creep.
One coordinator can realistically own:
- ~150 accounts solo
- Up to 250 with support roles in place
The HRT clinic we grew from $1M to $4M in 4 years
…is the operational reference point for this staffing model.
Should I hire a Filipino VA for patient follow-up in my cash-pay HRT clinic?
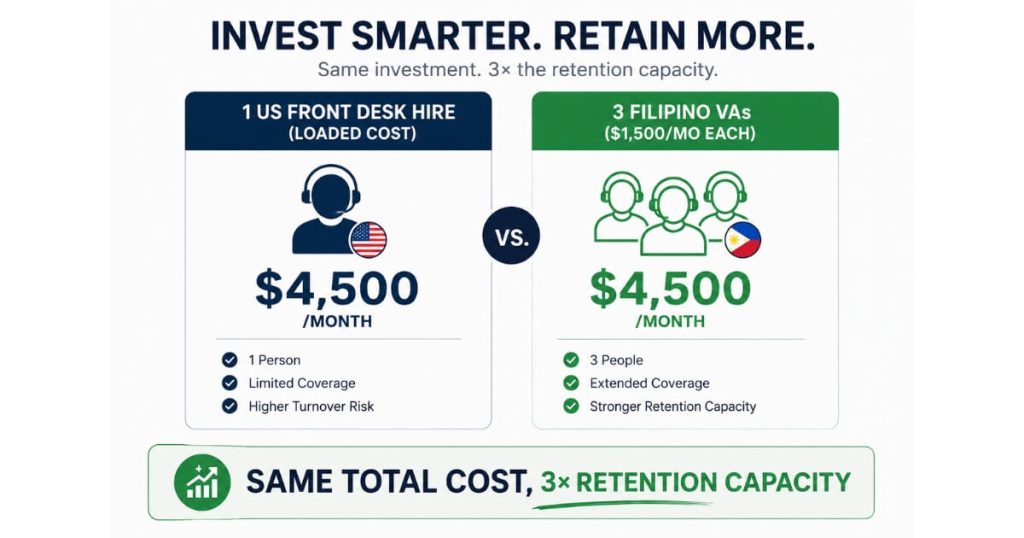
Yes — a medically-trained Filipino VA from a service like Medva costs roughly $1,500/month, runs about a third the loaded cost of a U.S. front-desk hire, and can be plugged directly into the team’s Microsoft Teams + Go High Level setup so the on-site staff treats them as part of the practice.
The staffing math surprises most clinic owners.
Three full-time Filipino VAs cost less than one U.S. front-desk hire.
For a growing cash-pay clinic where office space is already tight (Prime Medicine’s most recent hire sits in the IV room because the front office is full), the VA model is the only way to add retention capacity without leasing more square footage.
The VAs:
- Work U.S. hours
- Speak English
- Often have healthcare-specific training
…especially when sourced through Medva or a similar healthcare-focused provider.
The specific use case
The VA:
- Reads each provider note as it’s submitted
- Confirms whether the patient has a future appointment booked
- Creates follow-up tasks in Go High Level if they don’t
- Messages the patient via text or email
- Escalates to the on-site MA when needed
The on-site team no longer has to do the reading-and-triaging work manually.
Outreach structure options
The clinic owner decides:
- Whether the VA messages patients directly using an Americanized name
OR - Whether the VA only creates tasks for the U.S. team to complete
Both work.
Outreach-by-VA scales further.
Task-creation-only feels more comfortable for some clinics.
Either way:
The VA becomes the workflow’s central nervous system.
What’s the right workflow when an EMR like Dr. Chrono won’t trigger follow-up tasks automatically?
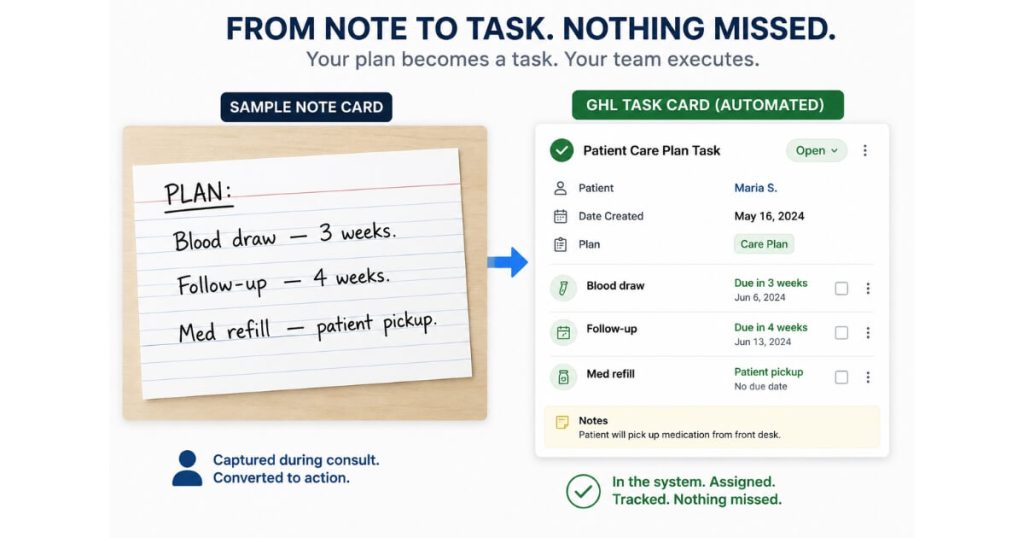
Use Go High Level as the source of truth for tasks, and have a VA listen to or read every visit note as soon as it’s submitted and create the GHL follow-up task manually based on the note’s instructions.
Most EMRs in the cash-pay space:
- Dr. Chrono
- Hint
- Cerbo
…do not cleanly fire structured follow-up tasks from provider free-text notes.
The workaround
The VA:
- Reads the provider note
- Translates the instructions into scheduled tasks inside GHL
- Sets the dates manually
Example:
“Blood draw in 3 weeks, follow-up in 4 weeks”
…becomes:
- Blood draw task
- Follow-up scheduling task
- Reminder cadence
The team and the outreach VA both work from the GHL task list as the single source of truth.
Why this works better than forcing EMR automation
Because 3 out of 10 visits are outliers.
The provider might:
- Change the protocol mid-visit
- Give a custom timeline
- Adjust the plan manually
Rigid automations break on outliers.
A trained VA does not.
The VA is the:
- Intelligence layer
GHL is the:
- Task layer
For clinics with partial EMR notification capabilities, the notification simply becomes the trigger the VA monitors.
If the EMR cannot trigger notifications cleanly, the VA polls completed visits daily.
Either way:
The workflow lives in GHL, not the EMR.
How tight should the provider’s note be for the follow-up VA to work off it?
Tight.
The provider’s plan needs to follow a deterministic structure like:
“Blood draw in 3 weeks, follow-up in 4 weeks, med refill — patient pickup”
…so the VA can convert it into tasks with zero judgment calls.
This is one of the small operational disciplines that quietly multiplies revenue.
Tight notes:
- Faster task creation
- Fewer missed follow-ups
- Cleaner scaling
Vague notes:
- Clarifying questions
- Generic tasks
- Missed instructions
Multiply that across:
- 30 visits per day
- Multiple providers
- Hundreds of active patients
…and the difference becomes massive.
Recommended provider note structure
Every plan section should include:
- Clinical task
- Labs
- Follow-up
- Medication change
- Timeline
- “3 weeks”
- “Before next visit”
- “As needed”
- Ownership
- Patient pickup
- Clinic ships
- Patient self-schedules
The clinic should standardize this across providers and audit it weekly during rollout.
How do I write a scorecard or SOP for a patient follow-up coordinator (or VA) before hiring?
Use a 4 R’s framework:
- Role
- Responsibilities
- Requirements
- Results
Write the document before the hire, and have a senior team member do the role manually for two weeks first so the SOP reflects real-world workflow.
The 4 R’s scorecard
Role
- Patient Follow-Up Coordinator
- Retention VA
- Client Service Coordinator
Responsibilities
- Read every completed provider note
- Confirm next appointment status
- Create GHL tasks if missing
- Message patients per cadence
- Escalate to on-site team when needed
- Track touches across assigned patients
Requirements
- GHL access
- Microsoft Teams access
- Dr. Chrono read-only access
- Medva training
- English fluency
Results
- % of patients with future appointment booked
- Follow-up completion rate
- Message response rate
- Member retention rate
- Churn rate
Why the “manual first” step matters
Most clinics skip this.
Then the SOP breaks immediately because:
- Edge cases weren’t documented
- Real-world workflow differed from assumptions
When a senior team member runs the role manually first:
- The SOP becomes reality-based
- The team can record training videos
- The VA learns from actual scenarios
…built its inside-sales scorecard the same way:
- 4 R’s
- Manual workflow first
- Then delegation
The scorecard also makes the role replaceable.
If the first VA doesn’t work out:
The clinic does not restart from scratch.
What’s the next step?
If your cash-pay HRT or functional medicine clinic has a patient list growing past 150 active members and you’re watching paying patients drift past their follow-up windows, book a strategy call.
In 60 minutes we’ll:
- Map the current note-to-task workflow
- Write the 4 R’s scorecard for the follow-up coordinator or VA
- Lay out the Medva (or equivalent) staffing structure
…built to scale to 250+ members without adding U.S. front-desk headcount.