How Should a Cash-Pay Functional Medicine Clinic Launch a Niched Productized Protocol Program (Like an “Aviator Protocol” for Pilots)?
A productized protocol program — one named protocol, targeted at one specific patient profile, with a defined sequence of labs, supplements, and provider interactions — is one of the strongest growth moves a cash-pay functional medicine clinic can make. Done right, it stabilizes revenue and gives the clinic a memorable wedge into a niche audience. Done wrong, it eats a year of marketing spend chasing supplement subscriptions that pay 40% margin while the actual program offer never converts. Here’s the FAQ on the launch order that works.
What is a niched / productized protocol program at a cash-pay functional medicine clinic and why does it work?
A productized protocol program takes the clinic’s standard functional medicine assessment-and-protocol model and re-packages it for a specific patient profile:
- Pilots
- Firefighters
- Perimenopausal women
- Executive endurance athletes
…with:
- A memorable program name
- A specific result promise
- A defined 3–6 month sequence of labs, supplements, and provider touchpoints
The reason it works is positioning.
A patient searching for:
“functional medicine in New Braunfels”
…sees ten clinics that all sound interchangeable.
A pilot searching for:
“jet lag fatigue functional medicine pilots”
…sees one clinic that’s clearly built around the problem they actually have — and that clinic now has a structural reason to:
- Charge more
- Convert better
- Differentiate from competitors
An HRT clinic we grew from $1M to $4M in 4 years
…did exactly this on the hormone side:
- Specific patient profiles
- Named protocols
- Predictable touchpoints
- Clear 12-month outcome promise
Example: The Aviator Protocol
For Elive Health, the productized program is the:
“Aviator Protocol”
Built around:
- Pilots
- Circadian rhythm correction
- Detox pathway support
…and designed to be sold through a niche social audience.
(The founder’s husband is a pilot, which gives the clinic credible access to the community.)
The clinic’s core service didn’t change much.
The:
- Audience
- Name
- Offer language
…did.
That’s the whole move.
How should a cash-pay functional medicine clinic name and position a niched protocol program?
Name it after the patient identity:
- Aviator
- First Responder
- Perimenopause Reset
…and position it around the patient’s most specific pain point — not around the clinical category the protocol falls under.
The naming test
Someone in the niche should immediately think:
“Oh, that’s for me.”
Good example:
Aviator Protocol
Bad example:
Comprehensive Functional Medicine Program for Aviation Professionals
Why?
Because the second version is:
- Too long
- Too generic
- Written by a clinician instead of a marketer
The shorter identity-first name does the heavy lifting in:
- Social media
- Word-of-mouth
- Referral conversations
Positioning rule #1:
Lead with the most-specific pain point the niche shares.
Not the clinical mechanism.
Pilots care about:
- Jet lag
- Irregular sleep
- Schedule chaos
- Recovery under stress
They care far less about:
- Circadian rhythm optimization
- Detox pathways
…because those are the internal mechanics, not the patient-facing promise.
Better marketing angles:
- “Sleep that recovers in a single-night layover”
- “Recover from a 14-hour rotation by morning”
The clinical explanation happens later — on the discovery call.
Positioning rule #2:
Anchor the program to a face, not the clinic.
A productized protocol works hardest when there’s a credible voice attached:
- Founder
- Notable patient
- Clinical advisor
…did this by anchoring the protocol to the founder’s personal authority.
The niche audience trusts the person first.
The clinic second.
The program is downstream of that trust.
Should a cash-pay functional medicine clinic sell supplements as a standalone subscription or include them inside the program?
Include the supplements inside the program.
Selling supplements as a standalone subscription is:
“Stepping over dollars to pick up pennies.”
You do the marketing work to acquire a willing-to-pay customer…
…then sell them a 35–40% margin product instead of a high-LTV protocol.
The math
A supplement pack at:
- $149/month
- 40% margin
…pays the clinic about:
- $60/month profit
…while still carrying:
- Clinical responsibility
- Customer-service burden
- Fulfillment complexity
The same patient inside a productized protocol:
- $1,500–$3,000 entry
- Monthly clinical touchpoints
…produces 5–10× more value over the same period.
When supplement subscriptions DO work
They work for clinicians who already built:
- Podcast audiences
- YouTube audiences
- Social followings
In that case:
- Supplements are the OUTPUT of the audience
- Not the ENTRY POINT of the funnel
The Victoria-based functional medicine practice doing $13,000/month in supplement-pack subscriptions runs exactly that model.
For most cash-pay clinics still building an audience:
- Supplements should support the protocol
- Not replace the protocol
The right architecture
Supplements live inside the program as part of the protocol delivery.
The clinic can optionally offer:
- Pre-packaged convenience supplement packs
- Travel packs
- Existing-patient add-ons
But the supplements are not the core offer.

How does a cash-pay clinic build an offer for a brand new productized protocol program (without case studies yet)?
Run the protocol on 2–3 beta patients first.
At-cost or discounted.
In exchange for:
- Measurable results
- Testimonials
- Documentation rights
Then build the public offer around the outcomes those patients produced.
This is the step most clinics skip.
The wrong order
A clinic gets excited.
Then:
- Builds the landing page
- Writes ad copy
- Runs traffic
…before a single patient completes the protocol.
Result:
- Generic claims
- Weak conviction
- Low conversion rates
- High ad costs
The program quietly dies.
The correct order
- Recruit 2–3 ideal-fit beta patients
- Run the protocol at-cost or discounted
- Measure outcomes obsessively
- Document everything
- Build marketing around actual outcomes
For the Aviator Protocol:
- Founder spouse who is a pilot
- Two additional recruited pilots
Measure:
- Sleep hours
- Energy ratings
- Recovery time
- Lab markers
After 60–90 days:
The clinic now has:
- Specific stories
- Specific results
- Specific language
Examples like:
“How this pilot went from sleeping three hours a night to eight hours and feeling fully recovered.”
Now:
- Ad copy becomes specific
- Landing pages become believable
- Conversion rates improve
The beta stage also validates whether the protocol is actually effective.
Better to discover a weak protocol with three beta patients…
…than after $20,000 in paid ads.
Should a cash-pay functional medicine clinic run paid ads on a new productized protocol program before it has case studies?
No.
Run paid ads only after:
- 1–2 documented case studies exist
- Outcome language is proven
- Organic content already resonates
Then start small:
- $40–$50/day
…to test:
- Creative
- Offer language
- Positioning
The temptation to run ads early is understandable.
But paid traffic amplifies the weakest part of the funnel.
If the:
- Landing page
- Messaging
- Offer
…are vague, paid traffic becomes expensive noise.
The only exception
If the clinic already runs profitable ads on an established offer…
…the new protocol can sometimes be added as:
- An additional ad set
- Inside an existing campaign architecture
That is not really a true launch.
It’s an expansion of an already-working machine.
Correct launch order
- Beta patients
- Documented outcomes
- Offer language built from outcomes
- Organic social content
- $40–$50/day paid ads
- Scale only after booked-patient cost is healthy
Each stage costs less than the next.
Each stage generates the data needed for the next stage.
Skipping the beta stage skips the data that makes the ad stage work.
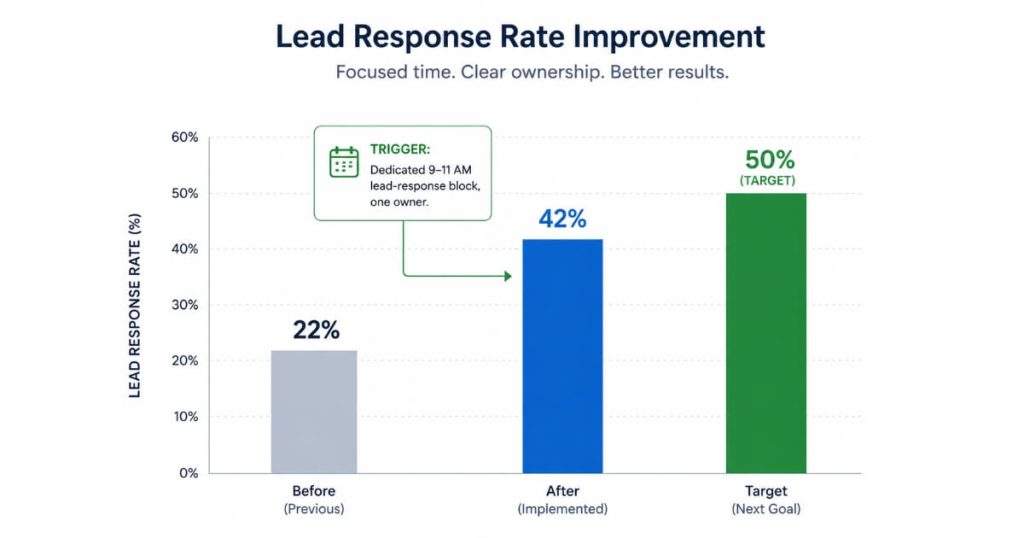
How does a cash-pay clinic raise its lead conversion rate from 22% to 50% on a new productized program?
Assign:
- One specific person
- One specific time block
- One specific responsibility
…and make it non-negotiable.
The Elive Health clinic moved its lead-to-scheduled-consult conversion rate from:
- 22%
…to: - 42%
…inside four weeks by doing one thing:
Christy owned the:
9 AM–11 AM lead-response block every weekday.
That was her only job during that window.
No:
- Ad changes
- Funnel rebuilds
- Script rewrites
Just:
- Faster response
- More consistent follow-up
Why this works
Website leads decay by the minute.
A lead contacted within 10 minutes converts at multiples of the rate of a lead contacted the next day.
When lead handling belongs to:
“Whoever happens to be free”
…conversion rates stay low.
When one person owns the process:
- Response time drops
- Pattern recognition improves
- Follow-up consistency improves
- Conversion rate rises
The target benchmark
50% lead-to-scheduled-consult conversion.
Most clinics that hit it have:
- One named lead owner
- A written follow-up cadence
- CRM source tagging
- Consistent response windows
Standard cadence example
- Call
- Text
- Call back in 24 hours
- Text again in 72 hours
The Elive Health team implemented:
- The 9–11 AM lead block
- CRM source tagging
…in the same month.
Conversion moved:
- 22% → 42%
50% is the realistic next milestone.
What’s the next step?
If your cash-pay functional medicine clinic is sitting on a strong idea for a niched protocol program:
- Aviator
- Perimenopause Reset
- First Responder
- Athlete Recovery
…and you’re trying to figure out:
- Whether to lead with supplements
- How to recruit beta patients
- When to run paid ads
- How to structure the offer
…book a strategy call.
In 60 minutes we’ll map:
- The launch order
- Offer architecture
- Case-study recruiting plan
- Lead-conversion block
…then build it over the next 30–60 days.