How Does a Cash-Pay Concierge HRT Clinic Know It’s Time to Raise Prices? (Booked Out 3 Months, Front Desk at Capacity, 200+ Members)
A cash-pay concierge HRT clinic that’s hit 200+ active members, is booked out three months on the lead provider’s calendar, and just hired its second front desk staffer to keep up with doubled inbound call volume is sending the same signal three different ways: demand is now ahead of capacity. Adding more marketing makes this worse, not better. The right next move is a controlled price increase on new patients — and a hard re-enforcement of who does what inside the clinic. Here’s the FAQ on how to execute that without losing momentum.
When should a cash-pay concierge HRT clinic raise its membership prices?
Three signals fire together:
- The lead provider is booked out 90 days or more
- Inbound call volume has roughly doubled inside a year
- The front desk has hit capacity even after a second hire
When all three are present, the clinic is no longer leaving money on the table by holding prices flat — it’s leaving money on the table by NOT raising them.
Demand is exceeding the clinic’s ability to deliver at current price points, and the patients booking in today are doing so partly because they know the slot is scarce. That’s the moment economics says to raise the price.
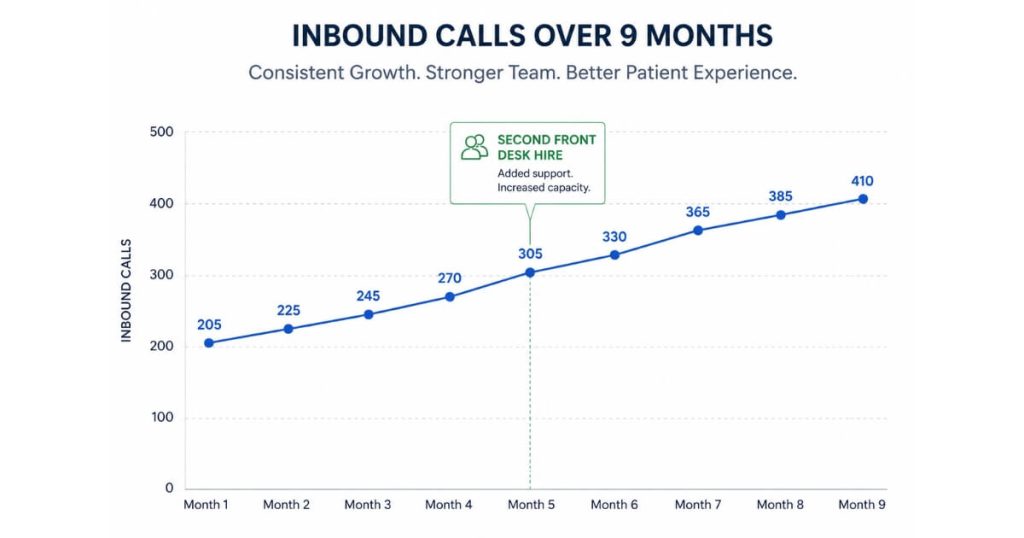
We’re working with a concierge HRT clinic right now that:
- Went from roughly 200 inbound calls in January to roughly 400 inbound calls in September
- Sits at over 200 active members
- Is booked out until January for the founder-provider
It just hired:
- A nurse practitioner (Holly) who’s booked out through November
- A second front desk hire (Brianna) to support the existing front desk lead (Shelby)
All three signals fired.
We raised new-patient pricing $50 across the membership tiers and labs the same week.
The point isn’t to raise prices for the sake of raising them.
The point is that when the clinic is operating at the absolute limit of its current capacity and the wait list is real, price is the only lever that turns excess demand into the resources required to add more capacity.
How much should a cash-pay concierge HRT clinic raise prices?
About $50 a month across each membership tier, plus an equivalent bump on the initial-labs line, for new patients only.
The pattern that works for cash-pay HRT memberships is:
- Small
- Defensible
- Applied across the board
For the Heel-MD style clinic running:
- Base memberships at $300
- A more comprehensive tier at $350
…the move is to:
- $350
- $400
…respectively.
Labs price moves up about $50 too — initial labs jumping from breaking-even to net-positive on the unit economics by the time you net out the nurse’s time on the blood draw.
Why $50 and not $100?
Concierge HRT memberships have unusually high retention and low price-elasticity at the bottom of the funnel.
The patient already worked through whether to spend $300/month or $400/month before they ever called the clinic, and the $50 delta is invisible compared to the gap between:
- “Do this”
- “Don’t do this”
A $100 jump, on the other hand, starts to look like a different positioning conversation:
- Premium-tier
- Higher-touch
…and that’s not the right experiment to run while the front desk and provider calendar are both being rebuilt.
The HRT clinic we grew from $1M to $4M in 4 years
…ran exactly this discipline:
- Small, regular price moves on new enrollments
- Never on existing members
- Additional revenue funneled into hiring providers and a second clinical lead
For family or couple tiers, the same $50 logic applies to each enrolled person — so a couple membership ends up about $100 more per month than it did pre-increase.
Patients enrolling at the family tier are explicitly opting into a higher-touch experience and tend to absorb the per-person increment without friction.

Should an existing patient at a cash-pay HRT clinic be subject to a price increase?
No.
Existing members keep their original rate; the price increase applies only to new enrollments.
This is non-negotiable in the concierge HRT model and most cash-pay membership models in general.
The patient:
- Enrolled at a stated price
- Set up auto-billing
- Built the membership into their household budget
Adjusting that price after the fact — even with notice — burns trust at the exact moment the clinic needs goodwill to fund referrals and avoid churn.
The math also doesn’t work:
Any short-term revenue lift from re-pricing existing members gets dwarfed by:
- The churn it triggers
- The referral velocity it kills
The clean version of the policy:
“We’re adjusting our pricing for patients starting after [date]. Your rate is locked.”
Tell the team to say it that way on the phone the first time a prospect asks why a friend got in for less.
The honesty is the marketing.
If a specific membership tier was deliberately underpriced relative to what the clinic delivers — for example, if a progesterone-heavy patient is costing $85–$90/month in drug pass-through against a $350 membership and the margin no longer makes sense — the right fix is not to re-price the existing patient.
The right fix is to:
- Tighten the protocol design
- Adjust the drug source
- Modify dose or supply window
- Apply the price update to new patients on that profile going forward
What’s the right call when a cash-pay clinic’s inbound call volume doubles in 9 months?
Hire the second front desk role before the existing front desk lead burns out — and make sure the new hire’s lane is explicit and protected from clinical creep.
When inbound calls grow from ~200 to ~400 in nine months at a clinic with one front desk staffer, the existing person is already:
- Missing GHL messages
- Missing call-backs
- Rolling tasks forward into the next day
The pattern shows up in three places:
- Unread message queues climbing past 1,000
- Message threads verbally responded to but never marked-read
- The front desk lead doing back-office prep because there’s no one else to do it
The mistake most cash-pay clinic owners make is hiring the second front desk role as:
“An extra pair of hands”
That framing produces overlap — both people end up doing the same job badly.
The right framing is:
“The second hire owns a specific lane the first hire can’t cover anymore.”
Examples:
- Inbound message queue
- New-patient intake flow
…while the first hire stays focused on what they already do well.
It also matters who picks up the slack while the new hire ramps.
If the front desk is shared with the clinical team during the training period and the new hire ends up:
- Drawing peptides
- Setting up IVs
…because the nurses are busy, the role permanently drifts.
The first three weeks set the role definition forever — defend the lane from day one.
How do you stop the new front desk hire from getting pulled into nurse-level back-office work?
Tell the nurses, explicitly, that:
- All draws and clinical prep are theirs
- The front desk hire is not available to cover those tasks
- The front desk role stays at the front desk even when nurses are busy
The dynamic is predictable:
A new front desk hire who has:
- Any clinical background
- A willingness to help
…will get asked to:
- Draw up peptides
- Prep injections
- Step into IV rooms
The nurses are grateful.
The new hire feels useful.
Within a month, the front desk role has eroded into a hybrid that no longer covers the inbound call queue.
The owner finds out only when:
- Leads stop being answered
- The second hire burns out trying to be in two places
The fix is verbal and operational, not policy-document.
First conversation
With the front desk lead:
“Brianna stays at the front. If a nurse needs a draw done, the nurse does it. If a nurse can’t get to a draw, the patient waits or the appointment moves.”
Second conversation
Have the same conversation with the nurses directly.
Third operational move
Build the front desk hire her own desk physically at the front.
Even physical position protects the role.
If clinical capacity genuinely is the constraint, the fix is more nursing hours — not stealing front desk capacity.
The economics of a cash-pay clinic with:
- 200+ members
- 400 inbound calls a month
…support paying for an extra nursing shift.
They collapse if the front desk goes down.
Why does adding a nurse practitioner not always solve a cash-pay clinic’s capacity problem (right away)?
Because new providers ramp slowly.
They:
- Start with hesitancy about taking new patients
- Need help with case plans
- Inherit patient trust gradually
Patients often hold out for the founder-provider until trust transfers over.
A nurse practitioner joining a 200+ member concierge HRT clinic typically books out within 6–8 weeks because:
- The existing patient base is hungry
- The founder-provider is already booked into next year
But the NP’s case-plan throughput is slower than the founder-provider’s for the first 90 days.
The booking conversation requires a script the new patient coordinator can run:
“You’re both of our patients — she’ll see you first, and she reviews every case with the founder before any protocol changes.”
That language alone changes conversion meaningfully.
We’ve watched it move concierge HRT clinics from:
- “Patients won’t see the new provider”
…to:
- “Patients are signing up regardless of who they see first”
…inside a month.
The owner-side work during the NP ramp is two things:
1. Protect the NP’s calendar
Low-value tasks should not consume the provider’s day.
Examples:
- Existing patient peripheral questions
- Administrative cleanup
These belong to:
- The founder
- The VA
…not the new provider.
2. Give the NP a founder review window
End-of-day case-plan review with the founder is mandatory during the first 90 days.
…used exactly that case-review discipline.
Every new provider’s first 90 days were:
- Structured around founder co-review
- Then graduated to autonomy
The clinic should expect a new NP to be unit-economics-positive by month four or five — not month one.
The provider ramp is real.
Holding pricing flat in the meantime — when the founder is booked three months out and demand keeps growing — is a hidden subsidy from the clinic to its new patients.
A small price increase right before the NP comes fully online closes that subsidy.
What’s the next step?
If your cash-pay concierge HRT or functional medicine clinic is:
- Booked out more than 60 days on the lead provider
- Seeing inbound calls grow sharply in the last 6–12 months
- Watching the front desk show signs of strain
…book a strategy call.
In 60 minutes we’ll:
- Review the membership pricing structure
- Review the front desk role definition
- Review the NP ramp plan
- Map exactly what to change in the next 30 days