How Does a Cash-Pay Clinic Use a Patient Success Coordinator to Turn the 6-Month Program Into Memberships?
A cash-pay clinic that sells a 6-month program and then hopes the patient renews is leaving its single biggest revenue lever untouched. The clinics that convert program patients into long-term members assign a dedicated patient success coordinator, hand the patient off warmly the moment they enroll, book every next touchpoint before the current one ends, and use documented progress to make the membership feel like the obvious next step. Here’s the FAQ on how that system works, built from a real concierge clinic’s patient-journey playbook.
How Do You Get 6-Month Program Patients to Convert Into Memberships?
Assign a dedicated patient success coordinator, hand the patient off to them warmly at enrollment, book every next call before the current one ends, and use their documented progress to frame the membership as a logical continuation — not a new sale.
The renewal is won across the whole six months, not in the closing conversation.
Most clinics treat the 6-month program and the membership as two separate sales, then wonder why renewal rates are low.
The fix is to design the entire program as a relationship that obviously continues.
One person — the patient success coordinator — owns the patient experience from enrollment through month six.
Their responsibilities include:
- Preparing for every interaction
- Tracking progress against real scores
- Leading a “what’s next” conversation in months five and six
- Framing continuing care as the natural choice for someone who’s seen results
By the time the membership comes up, it isn’t a pitch; it’s the next chapter.
That retention engine is what powers high-lifetime-value clinics like an HRT clinic we grew from $1M to $4M a year on 250 members paying $1,000 a month.
What Is a Warm Handoff and Why Does It Matter So Much?
A warm handoff is a short, scheduled video intro — within about 24 hours of enrollment — where the provider personally introduces the patient to their coordinator and positions them as “your person for the next six months.”
It transfers trust from the provider to the coordinator so the relationship doesn’t depend on the doctor’s calendar.
The handoff is the hinge the whole system turns on.
After:
- The discovery
- The initial consult
- The treatment plan
The provider doesn’t just disappear into the next appointment.
Within 24 hours, there’s a brief video call where the provider says, in effect:
“This is your coordinator, she’s your person for the next six months.”
Then the provider steps off and the coordinator immediately books the next touchpoint.
That single move does two things:
- It makes the patient feel cared for at the most fragile moment (right after they’ve paid).
- It transfers trust so the patient will engage with the coordinator instead of waiting for the busy provider.
Without the warm handoff, the coordinator is a stranger leaving voicemails; with it, they’re the patient’s trusted guide.

What Is BAMFAM, and How Does It Eliminate No-Shows and Ghosting?
BAMFAM stands for “Book A Meeting From A Meeting” — the coordinator never ends an interaction without the next one already scheduled.
It replaces random voicemails and chasing with a continuous, pre-booked sequence of touchpoints.
The reason program patients drift and ghost is that the clinic leaves the next contact to chance:
- A voicemail here
- A “we should check in” there
BAMFAM removes the gap entirely.
Before any call or visit ends, the coordinator books the next one on the calendar with the patient still on the line.
The result:
- No more cold outbound voicemails into the void
- Every touchpoint was scheduled at the previous touchpoint
- The patient always knows when they’ll talk next
- The coordinator always has a full calendar of committed conversations
- Nobody falls through the cracks between month two and month five
Which is exactly where most renewals are lost.
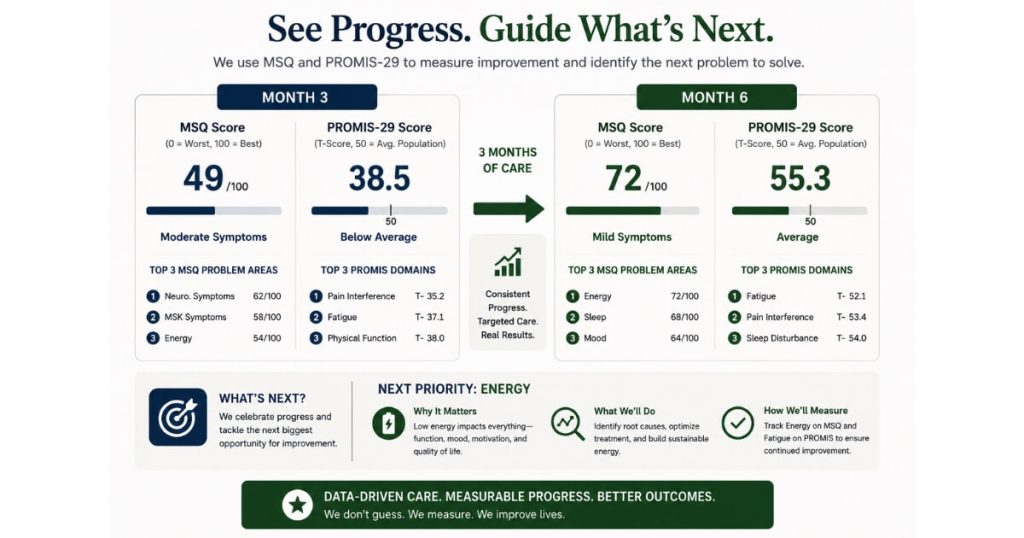
How Do I Use MSQ and PROMIS Scores to Drive Renewals?
Capture standardized symptom and quality-of-life scores (like the MSQ and PROMIS-29) at intake, three months, and six months, then show the patient their own side-by-side improvement — and the next problem area still worth solving.
Documented progress is the most honest renewal argument there is.
Patients forget how bad they felt when they started.
Objective scores fix that.
By administering the MSQ and PROMIS-29 at:
- Intake
- Three months
- Six months
The coordinator can sit a patient down and show them, in their own numbers:
“Here’s where you’ve improved.”
And then:
“Here’s what’s still not where you want it.”
Maybe:
- Energy is dramatically better
- Sleep is dramatically better
- The joints are still a 9 out of 10
Which opens a natural conversation about a regenerative or peptide path going forward.
The data does the persuading:
- It proves the program worked
- It identifies the next goal
So continuing care is obviously worthwhile.
This is the same progress-driven approach behind a functional and longevity medicine clinic we helped grow website leads by 900% and inbound calls by 100+ per month.
How Should I Frame the Membership Conversation in Months Five and Six?
Frame it as a logical continuation of the progress the patient has already made — not a new purchase.
Lead with:
- Their documented improvement
- The problem still worth solving
Then present the membership as how they keep going.
The continuation conversation is led by the coordinator, not the provider, and it’s built entirely on what the patient already experienced.
The coordinator:
- Opens with the progress data.
- Names the remaining goal the scores revealed.
- Frames the membership as simply how the patient keeps the momentum they’ve worked six months to build.
There’s no hard close because there doesn’t need to be one — a patient who can see they got measurably better and who has a clear next goal will continue.
The membership is positioned as the obvious vehicle for that, not as a separate thing they have to be sold on.
“New sale” energy kills renewals; “you’ve come this far, here’s how we keep going” energy wins them.
How Should I Measure and Manage a Patient Success Coordinator?
Measure them on conversations had, not outbound attempts made, and shift their role from “checking in” to coaching and prescribing the patient’s next steps.
What you measure is what the coordinator optimizes for.
If you grade a coordinator on outbound call volume, you get:
- A lot of voicemails
- Very little engagement
Grade them on real conversations — meaningful touchpoints with patients — and the behavior changes.
Their one-on-ones with leadership should move from pure operations:
“Did you make the calls?”
To higher-value discussions:
- Case reviews
- “What cool thing are we giving patients this month?”
The goal is a coordinator who shows up to every interaction with:
- Fresh value
- A recommendation for the next step
Rather than a glorified appointment reminder.
A coordinator who coaches retains patients; a coordinator who merely checks in loses them.
This is one of the most overlooked components of a predictable patient acquisition system. The clinics that grow most consistently don’t just focus on generating new leads—they build processes that maximize retention, renewals, and lifetime value after the patient enrolls. When a patient success coordinator is responsible for guiding patients through measurable progress and into continued care, the practice becomes less dependent on constantly replacing lost patients with new ones.
FAQs About the Patient Success Coordinator Role
How Do I Convert 6-Month Program Patients Into Long-Term Members?
Assign a dedicated patient success coordinator who owns the patient from enrollment, hand the patient off warmly at the start, book every next touchpoint before the current one ends, and use documented progress to frame the membership as a logical continuation rather than a new sale.
What Is a Warm Handoff in a Cash-Pay Patient Journey?
A short scheduled video call within about 24 hours of enrollment where the provider personally introduces the coordinator as “your person for the next six months.” It transfers trust from the provider to the coordinator so the relationship doesn’t depend on the doctor’s calendar.
What Does BAMFAM Mean?
“Book A Meeting From A Meeting” — the coordinator schedules the next touchpoint before ending the current one. It replaces random outbound voicemails with a continuous, pre-booked sequence so patients don’t ghost or fall through the cracks.
How Do MSQ and PROMIS Scores Help With Retention?
Capturing them at intake, three months, and six months lets the coordinator show patients their own side-by-side improvement plus the next problem area still worth solving. The objective data proves the program worked and makes continuing care obviously worthwhile.
How Should I Measure a Patient Success Coordinator?
On conversations had, not outbound attempts made. Shift the role from “checking in” to coaching and prescribing next steps, so the coordinator brings fresh value to every interaction instead of acting as an appointment reminder.
What’s the Next Step?
If your clinic sells a 6-month program and then hopes patients renew, you’re leaving your highest-margin revenue to chance. A patient success coordinator — warm handoff, BAMFAM booking, progress-data reviews, and a continuation conversation built on results — turns program patients into members who stay for years.
If you want help designing the role, the handoff, and the 6-month journey for your specialty, that’s the conversation to book. We’ll map your patient journey and show you exactly where renewals are slipping away.