When Should a Cash-Pay Clinic Add Capacity vs Raise Prices?
It is the best problem a cash-pay clinic can have.
It is also the one most owners handle badly.
Demand finally exceeds supply.
The founder-provider is booked out for months.
And marketing is working better than the calendar can absorb.
The instinct is to hire.
Sometimes that is right.
Just as often, the real answer is to raise prices, route demand off the founder, and protect the value of the team you already have.
This is the decision framework, pulled from the field: the utilization signals that tell you which problem you actually have, the margin math, and the patient-experience tests that keep scaling from eroding what patients pay for.
How do I know if my cash-pay clinic should add capacity or raise prices?
Read your utilization and your lead flow together.
Then ask whether the constraint is the whole clinic or one named provider.
If the calendar is genuinely full for weeks out, your lead-to-booking conversion is healthy, and patients keep saying yes at your current price, you have proven demand and a supply problem.
Add capacity.
If patients drop out at the price conversation, the calendar has holes, or conversion is soft, raising prices is the cheaper, faster lever.
Hiring would only stretch thin demand across more empty slots.
The most common misread is treating “we are busy” as “we should hire” without checking who is busy.
We saw this exact situation at a Tampa Bay hormone and wellness clinic.
The founding doctor was booked into next quarter for new patients.
At the same time, a second provider had open slots that same week.
That is not a pure capacity problem.
It is a routing and pricing problem wearing a capacity costume.
The fix was not a third provider.
It was routing speed-motivated patients to the available provider, charging the same, and letting founder-loyal patients wait.
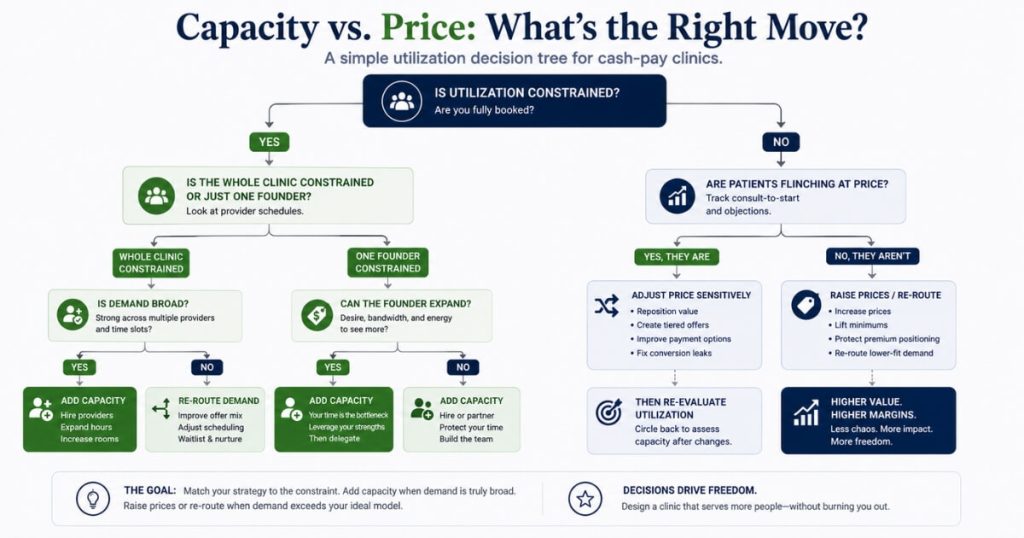
The clean rule:
- Add capacity when the whole clinic is constrained and demand is broad across providers.
- Raise prices when demand is narrow, concentrated on one person, or visibly price-insensitive.
Most clinics reach for the expensive lever first.
Reach for pricing and routing before you spend a dollar adding bodies.
For how acquisition, capacity, and pricing fit together, our guide to medical practice marketing is the hub for this topic.
What utilization signals tell me it is time to add capacity?
The clearest signal is a sustained booked-out window on your primary provider.
New patients cannot get in for four to eight weeks.
And the backlog is not clearing through cancellations.
That window has to be paired with a high conversion rate.
A full calendar built on slow-converting leads is fragile, not constrained.
Conversion is the proof the demand is real.
At the Tampa clinic, the team converted over half of website leads into booked appointments.
That was fourteen discovery calls booked out of twenty-one website leads in a single month.
When you are converting north of 50% and closing the calls you take, the constraint is hours, not interest.
That is when capacity actually pays back.
Then watch the leak: the prospect who wants speed and walks because the named provider has nothing until January.
A few are healthy scarcity.
A pattern is lost revenue and the trigger to add hours.
Run the math:
- Discovery calls per week
- Times close rate
- Times the share willing to see anyone rather than only the founder
Four discovery calls a week closing near 100%, with half choosing the available provider, lands around five to six new consults a week against your open slots.
When that number outruns your slots for 45 to 60 days running, you are out of runway.
Until then, you are managing routing, not buying capacity.

Should I charge less for a nurse practitioner or PA than for the MD?
No.
Charge the same for the same protocols, programs, and level of care.
Discounting the mid-level visit quietly tells the patient the care is worse.
A patient choosing between $500 with a “lesser” provider and $700 with the doctor will frequently pay the $700 and wait.
That is the precise opposite of what you want when the doctor is the bottleneck.
This is the single most important pricing decision when routing demand off a booked founder.
A price gap pays patients to doubt your team.
It also funnels everyone back toward the one calendar you cannot expand.
If protocols, programs, and outcomes are identical, the credential alone does not justify a different price.
The Tampa clinic moved to flat pricing.
That meant one $600 fee covering labs and the initial appointment, whether the patient saw the nurse practitioner or the doctor.
The choice was offered plainly:
See me now, or see the doctor and wait.
Same price across the board protects the perceived value of every provider on your roster.
It also removes the friction that pushes everyone toward the booked-out founder.
The only time a price difference makes sense is a deliberately positioned “see the doctor” premium tier you choose as strategy.
It should not be a discount that sneaks in through a credential and caps the capacity you just paid to build.
How do I add capacity without losing the patients who only want the founder?
Use the founder as the front door and a warm handoff to transfer ongoing care.
The most reliable move is to put the new provider on the discovery call.
That way, the patient builds the relationship with them first.
This is the inverse of the founder-attachment problem.
At the Tampa clinic, the front-line provider running the discovery calls was directly increasing her own patient load.
Prospects met and built rapport with her before “which provider” ever came up.
For existing patients attached to the founder, do not yank them.
Have the new provider sit in on follow-up consults.
Then make an explicit warm handoff:
“She is going to take over your care from here, and I will pop in from time to time.”
This is human nature.
People who built a relationship with the founder are not thrilled to be reassigned.
The warm handoff respects that while freeing the founder’s calendar.
And accept the split.
A real share of patients were referred specifically to the founder and want the founder.
Let them wait while everyone else routes to the faster, equally-priced option.
Offer the choice openly.
Patients like speed.
And at identical pricing, a predictable ratio self-selects into the open calendar.
That ratio is your routing engine.
Grow consults without losing the founder’s loyalists.
When does raising prices beat adding capacity?
Raise prices instead of hiring when demand is concentrated, price-insensitive, or you cannot cleanly expand hours.
If the bottleneck is one founder-provider who cannot or will not add hours, a price increase on that calendar can be the smarter move.
This is common.
A fully booked calendar is not the same as a willing one.
If a meaningful slice of demand insists on that person, a price increase rations the scarce time and lifts margin without a single hire.
The margin math favors price almost every time it is available.
Adding capacity carries cost and ramp time:
- Recruiting
- Onboarding
- Payroll
- Weeks before the new provider contributes
A price change is immediate.
And it drops straight to the bottom line.
When conversion is strong and patients are not flinching at the current number, the market is telling you that you are underpriced.
A price test is faster, cheaper, and lower-risk than a hire.
This is how a pain-management practice cut its insurance dependence in half and added over $40,000 a month in cash revenue by repricing and repositioning premium services rather than stacking on more volume.
The order of operations matters.
When the founder is the constraint and demand is loyal to the founder, use price to weed lower-value patients off that calendar before you spend on bodies.
Add capacity only once broad demand outstrips the whole clinic.
Do not add capacity just because the busyness is concentrated on one person you could charge more to see.
How do I protect the patient experience while scaling?
Protect it by keeping the founder as the visionary face while the team handles fulfillment.
And never let the booked-out calendar silently turn prospects away.
The best-case version of scaling is the founder becoming the figurehead and brand.
A capable team grows delivery behind the scenes.
That was exactly the trajectory the Tampa owner named as preferred: the doctor as visionary face, the team handling fulfillment so the business can grow.
That outcome is built, not wished for.
It requires front-end relationships.
Usually, those relationships start through whoever runs the discovery call.
It also requires a warm-handoff structure that makes the transition feel like an upgrade.
The clinics that pull this off remove the founder as the single point of delivery.
That is the same engine behind a practice that grew from $1M to $4M while removing the owners from day-to-day operations.
Capacity, pricing, and patient experience were solved together.
Then watch the leak points the way you watch utilization:
- A prospect who wants speed and cannot get the named provider
- A patient who senses the mid-level is “the cheap option”
- A handoff that feels like being passed off
Flat pricing, equal positioning, founder cameos in follow-ups, and a real front-end relationship with the new provider all close those leaks.
Done right, the patient experiences full availability and consistent care no matter which provider they see.
And scaling stops threatening what patients pay for.
FAQ’s About Adding Capacity vs Raising Prices
How do I know if my cash-pay clinic should add capacity or raise prices?
Read your utilization and your lead flow together.
If your provider’s calendar is genuinely full for weeks out, your lead-to-booking conversion is healthy, and patients are still saying yes at your current price, you have proven demand and a supply problem.
That points to adding capacity.
If patients are dropping out at the price conversation, your calendar has holes, or your conversion rate is soft, raising prices is the cheaper, faster lever.
Adding bodies would just spread thin demand across more empty slots.
The trap is reading “we are busy” as “we should hire” without checking whether the busyness is the founder-provider specifically or the clinic generally.
When demand is concentrated on one named provider booked into next quarter, while a second provider has open slots this week, you do not have a pure capacity problem.
You have a routing and pricing problem first.
Add capacity when the whole clinic is constrained and demand is broad.
Raise prices when demand is narrow, concentrated, or price-insensitive.
What utilization signals tell me it is time to add capacity at a cash-pay clinic?
The clearest signal is a sustained booked-out window on your primary provider.
New patients cannot get in for four to eight weeks.
And that backlog is not clearing through cancellations.
Pair that with a high conversion rate from leads to booked appointments.
If you are converting more than half of your website leads into booked appointments and closing the discovery calls, the demand is real.
The constraint is hours, not interest.
Watch for the moment your booked-out window starts costing you patients who will not wait.
That is the prospect who wants speed and walks because the named provider has nothing until January.
A few of those is healthy scarcity.
A pattern of them is lost revenue and the trigger to add hours or a provider.
Run the simple math:
- Discovery calls per week
- Times close rate
- Times the share who will see anyone, not just the founder
That gives you weekly new consults.
When that number exceeds your open slots for 45 to 60 days running, you are out of runway and need capacity.
Should a cash-pay clinic charge less for a nurse practitioner or PA than for the MD?
No.
Charge the same for the same protocols, programs, and level of care.
Discounting the mid-level visit tells the patient the care is worse.
A patient deciding between $500 with a perceived lesser provider and $700 with the doctor will often pay the $700 and wait.
If your nurse practitioner or PA delivers the same protocols and the same outcomes, a price gap is paying patients to doubt your team.
It also quietly caps the capacity you just built.
Same price across the board does two things at once.
It protects the perceived value of every provider on your roster.
And it removes the friction that pushes everyone toward the single booked-out founder.
The exception is a deliberately positioned “see the doctor” premium tier.
But that is a pricing strategy you choose on purpose.
It should not be an accidental discount baked into a credential.
How do I add capacity without losing the patients who only want to see the founder?
Use the founder as the front door and a warm handoff to transfer ongoing care.
The reliable move is to have the new provider run the discovery call.
That way, the patient builds the relationship with them first.
That is the opposite of the founder-attachment problem.
The patient never bonds exclusively to someone who has no availability.
For existing patients attached to the founder, do not yank them.
Have the new provider sit in on follow-up consults.
Then make an explicit warm handoff:
“Bailey is going to take over your care from here, and I will pop in from time to time.”
Accept that a real share of patients were referred specifically to the founder and want the founder.
Let them wait for that calendar.
Everyone else can be routed to the faster, equally-priced option.
Offer the choice openly:
See the founder and wait, or see the equally-qualified provider this week.
Patients like speed.
And a predictable ratio will self-select into the open calendar when the price is identical.
When does raising prices beat adding capacity at a cash-pay clinic?
Raise prices instead of adding capacity when demand is concentrated, price-insensitive, or you cannot cleanly expand hours.
If the bottleneck is one founder-provider who cannot or will not add hours, and a meaningful slice of demand insists on that specific person, a price increase on that calendar can do two things.
It rations the scarce time.
And it lifts margin without hiring.
Raising prices also wins when your conversion is strong and patients are not flinching at the current number.
That is the market telling you that you are underpriced.
A price test is faster and lower-risk than a hire.
Adding capacity carries real cost and ramp time.
A price change is immediate and drops straight to margin.
The order of operations matters.
When the founder is the constraint and demand is loyal to the founder, weed the lower-value patients out by charging more for that calendar before you spend a dollar adding bodies.
Then add capacity only once broad demand outstrips the whole clinic.
How do I protect the patient experience while scaling a cash-pay clinic?
Protect it by keeping the founder as the visionary face while the team handles fulfillment.
And never let the booked-out calendar silently turn prospects away.
The best-case version of scaling is the founder becoming the figurehead and brand while a capable team grows the delivery behind the scenes.
That requires building relationships on the front end.
Usually, that happens through whoever runs the discovery call.
It also requires a warm handoff structure that makes the transition feel like an upgrade rather than a downgrade.
Watch the leak points:
- A prospect who wants speed and cannot get the named provider
- A patient who senses the mid-level is “the cheap option”
- A handoff that feels like being passed off
Same pricing, equal positioning, founder cameos in follow-ups, and a front-end relationship with the new provider all close those leaks.
The goal is for the patient to experience full availability and consistent care quality no matter which provider they see.