What Are the Worst Lead Sources for a Cash-Pay Clinic in 2026 (and Why)?
Most cash-pay clinics do not have a marketing problem — they have a lead-source problem.
They are pouring money into channels that were never going to work for a high-ticket, high-LTV cash practice. Then they blame “marketing” when the appointments do not show.
The truth is that some lead sources are structurally rigged against you.
They sell you the wrong patient, optimize for the wrong number, and give you no way to fix them.
This is the field guide to the channels that quietly drain cash-pay clinics in 2026, why each one fails when you grade it honestly, and what to run instead.
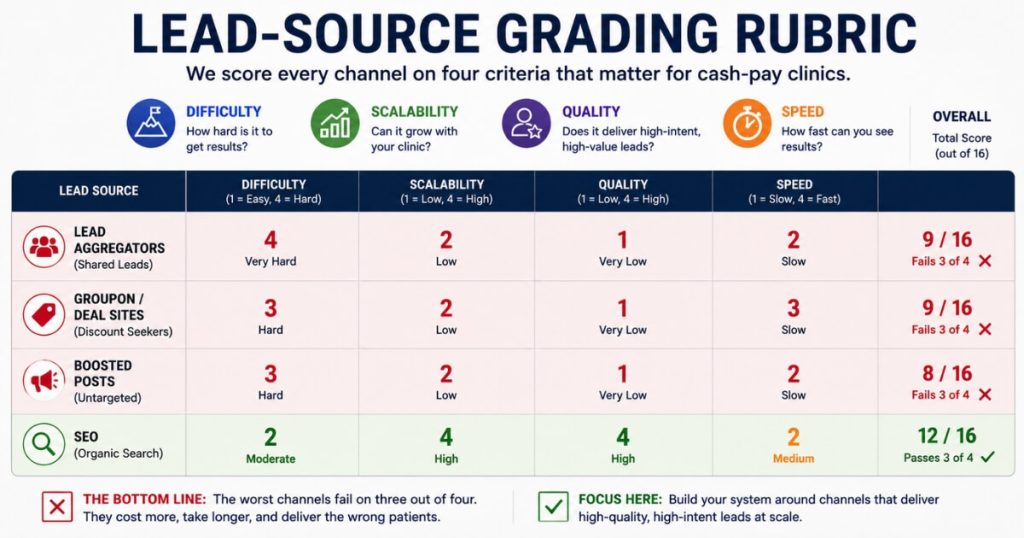
The grading rubric is simple: difficulty, scalability, quality, and speed. The worst sources fail it on three of the four.
What is the single worst lead source for a cash-pay medical clinic in 2026?
Shared lead aggregators are the worst lead source for a cash-pay clinic in 2026.
These are the pay-per-lead marketplaces that sell the same contact to four or five clinics at once.
The whole model is built against you.
The lead never asked for your clinic specifically.
They filled out a generic form on a portal, which means they are problem-aware at best and have no idea who you are.
They do not know your brand, your doctors, or your offer.
So the lead arrives cold and stays cold.
Worse, because the same lead is sold to multiple buyers, you are racing competitors to the phone.
The prospect is fielding five calls in an hour.
And the close rate craters no matter how good your front desk is.
You also cannot improve it.
Grade every channel on four things:
- Can you control and improve it?
- Can you scale it if it works?
- How ready-to-buy are the leads?
- How fast does it produce real results?
With an aggregator, you do not control the offer, the creative, the form, or the audience.
So the difficulty of fixing it is effectively infinite.
The scalability is zero the moment the shared pool runs dry.
The only thing it produces fast is a spreadsheet of cold names.
A high-LTV cash-pay clinic lives or dies on patient lifetime value.
And a lead who never chose you and is being called by four other clinics is the lowest-LTV lead you can buy.
For the full framework on which channels fit which treatment, our guide to medical practice marketing lays out the complete map.
Why are Groupon and daily-deal style discount platforms so bad for a cash-pay clinic?
Because deal platforms select for the exact patient a cash-pay clinic does not want:
The deal-seeker with no loyalty and the lowest possible lifetime value.
The entire reason cash-pay medicine works is patient LTV.
A hormone patient, a weight-loss patient, or a regenerative-medicine patient is worth thousands of dollars over time because they stay, rebook, and refer.
A daily-deal buyer is trained to do the opposite.
They buy the discount.
They take the service.
Then they disappear the moment the next discount appears at a clinic across town.
You are paying to acquire a patient who is structurally unlikely to ever pay full price or return.
That is the inverse of the business you are trying to build.
The economics are upside down before the patient walks in, too.
You hand the platform a cut of an already-discounted ticket.
So the front-end margin is gone on day one.
And it poisons your pricing.
Once a treatment has a public deal price, your full-cash patients feel overcharged.
Your team also starts quietly discounting to match.
There is a real difference between a strong introductory offer that you control and route into a proper service ladder, and renting a deal-platform audience that exists to chase the cheapest price in town.
The first builds a patient base.
The second builds a churn list.
Are untargeted boosted posts a bad lead source for a cash-pay clinic?
Yes — the boost button is one of the most reliable ways to waste a cash-pay clinic’s ad budget.
Boosting a post optimizes for cheap engagement, not for booked appointments.
It sends your money to the broadest, cheapest-to-reach audience the platform can find.
So you get likes, a handful of comments, and almost no patients.
Then the dangerous part happens.
You conclude that “Facebook does not work for us.”
But what actually failed was the boost button, not the platform.
Real Facebook and Instagram acquisition for a clinic is a completely different machine.
It runs on:
- An audience callout in the copy and image
- Static and video creative tested in parallel
- An aggressive offer
- A funnel that lands on a VSL or quiz
- A calendar with a credit-card hold to reserve the slot
- Fast follow-up
Most of the time, the cash needs to come in as fast as you are putting it out.
None of that exists in a boost.
The platform itself is excellent for the right offers.
Joint pain, neuropathy, body contouring, and any offer over three thousand dollars in front-end cash can all scale on Facebook when the offer, the ad team, and the follow-up are in place.
The boost button is not Facebook advertising.
It is the absence of it.
Orthobiologics Associates grew on a high-intent channel and converts inbound at a 79.4% rate — that is the gap between a real funnel and a boosted post.

Why do generic lead-magnet funnels and cheap PPL agencies underperform for cash-pay clinics?
Because they optimize for the cheapest possible lead instead of the most ready-to-buy patient.
For a high-ticket cash-pay clinic, those are opposite goals.
A generic e-book or “free guide” funnel run by a low-cost pay-per-lead agency collects emails from people who wanted the freebie.
Not the treatment.
Those leads sit far back in the awareness journey.
They are solution-aware at best, and often only problem-aware.
So they rarely convert into paid appointments.
The agency then reports a low cost per lead and calls it a victory.
But cost per lead is a vanity number.
The only metrics that matter for a cash-pay clinic are:
- Cost per booked appointment
- Lifetime value of the patient who actually shows up
A cheap lead that never books is infinitely expensive.
These funnels also tend to be templated.
They are often run identically across dozens of unrelated businesses.
So the messaging never matches your specific treatment, your demographic, or your local market.
Contrast that with channels you can actually control and improve:
- Your own SEO
- Your Google Business Profile
- Your owned social brand
With those channels, you can tune the offer, the landing page, and the follow-up until the economics work.
And the lead chose you on purpose.
That is the dividing line between a renter and an owner of demand.
It is also the single biggest predictor of whether a cash-pay clinic’s marketing compounds or just burns.
What should a cash-pay clinic run instead of these bad lead sources?
Run channels you own and can compound.
Start with SEO and your Google Business Profile.
Then add properly built paid acquisition matched to the treatment.
SEO is the single best way to build sustainable lead flow in a cash-pay clinic.
The leads are the most ready to buy and the most familiar with the business by the time they reach you.
And SEO compounds for years when paired with strong Google reviews and an established social brand.
The proof is in the numbers.
Eternity Health Partners built roughly $1.7M per year in revenue from SEO as a high-intent channel.
Orthobiologics Associates grew on SEO alone and converts inbound at a 79.4% rate.
That is exactly what high-intent, self-selected demand looks like next to a purchased aggregator list.
Those patients searched for the treatment, found the clinic, and chose it.
No race to the phone.
No shared list.
No discount-seeking.
From there, match paid channels to the treatment instead of chasing whatever is cheapest:
- TikTok for aesthetics
- Facebook for joint pain and higher-ticket cash offers run with a real funnel and fast follow-up
- Google and YouTube for product-aware search demand where people type the treatment in by name
The principle underneath all of it is to own the relationship and control the offer.
Do not rent an audience that never chose you.
Pick channels you can control, improve, and scale.
That is the whole grading rubric.
And it points away from every source on this list.
How do you grade a lead source before you spend money on it?
Grade every lead source on four criteria before you spend a dollar:
- Difficulty
- Scalability
- Quality
- Speed
Difficulty asks whether you can run and improve it yourself.
If you do not control the offer, the audience, the creative, and the funnel, you can never fix it when it underperforms.
That is precisely why aggregators and deal platforms are uncoachable.
Scalability asks whether getting it right means you can pour more money in and get more patients out.
A shared-lead marketplace caps the moment the pool is exhausted.
SEO and owned paid channels scale with investment.
Quality asks how ready-to-buy the leads are with a good offer.
A patient who searched for your treatment by name and chose your clinic is worlds ahead of a discount-seeker or a resold name.
Speed asks how fast it produces real booked appointments, not how fast it produces raw leads.
Run any channel through those four questions and the worst lead sources eliminate themselves.
Shared aggregators, daily-deal platforms, boosted posts, and templated cheap-PPL funnels are all:
- Hard to improve
- Impossible to scale
- Low in quality
- Fast only at generating noise
The good sources pass on all four because you own them.
You can improve the offer.
You can scale the spend.
The leads come pre-qualified by their own intent.
And over time, they produce booked, paid, returning patients.
The rubric is the whole game.
Apply it honestly and your budget stops leaking.
FAQ’s About the Worst Lead Sources
What is the single worst lead source for a cash-pay medical clinic in 2026?
Shared lead aggregators are the worst lead source for a cash-pay clinic in 2026.
These are the pay-per-lead marketplaces that sell the same contact to four or five clinics at once.
The whole model is built against you.
The lead never asked for your clinic specifically.
They filled out a generic form on a portal, which means they are problem-aware at best and have no idea who you are.
So quality is low by design.
Because the same lead is sold to multiple buyers, you are racing competitors to the phone.
The prospect is fielding five calls.
And the close rate craters.
You cannot improve it either.
You do not control the offer, the creative, the form, or the audience.
So the difficulty of fixing it is high and the scalability is zero.
The only thing it produces fast is a spreadsheet of cold names.
Judge every channel on four things:
- Can you control and improve it?
- Can you scale it if it works?
- How ready-to-buy are the leads?
- How fast does it produce results?
Aggregators fail three of the four.
The contrast that matters is simple.
A high-LTV cash-pay clinic lives or dies on patient lifetime value.
And a lead who never chose you and is being called by four other clinics is the lowest-LTV lead you can buy.
Why are Groupon and daily-deal style discount platforms so bad for a cash-pay clinic?
Because deal platforms select for the exact patient a cash-pay clinic does not want:
The deal-seeker with no loyalty and the lowest possible lifetime value.
The entire reason cash-pay medicine works is patient LTV.
A hormone, weight-loss, or regenerative patient is worth thousands over time because they stay, rebook, and refer.
A Groupon buyer is trained to buy the discount and leave when the next discount appears somewhere else.
So you pay to acquire a patient who is structurally unlikely to ever pay full price or come back.
You also hand the platform a cut of an already-discounted ticket.
So the front-end economics are upside down before the patient even walks in.
It poisons your pricing too.
Once a treatment has a public deal price, your full-cash patients feel overcharged.
Your team also starts discounting to match.
There is a difference between a strong introductory offer that you control and route into a real service ladder, and renting a deal-platform audience that exists to chase the cheapest price in town.
The first builds a patient base.
The second builds a churn list.
Are untargeted boosted posts a bad lead source for a cash-pay clinic?
Yes — the boost button is one of the most reliable ways to waste a cash-pay clinic’s ad budget.
Boosting a post optimizes for cheap engagement, not for booked appointments.
It sends your money to the broadest, cheapest-to-reach audience rather than to people likely to buy a treatment.
You get likes, a few comments, and almost no patients.
Then you conclude that Facebook does not work.
But what actually failed was the boost button.
Real Facebook and Instagram acquisition for a clinic is a different machine entirely.
It uses:
- An audience callout in the copy and image
- Static and video creative tested in parallel
- An aggressive offer
- A funnel that lands on a calendar with a credit-card hold to reserve the slot
- Fast follow-up
None of that exists in a boost.
The platform itself is excellent for the right offers.
Joint pain, neuropathy, body contouring, and any offer over three thousand dollars in front-end cash can all scale on Facebook when run properly with fast follow-up.
The boost button is not Facebook advertising.
It is the absence of it.
Why do generic lead-magnet funnels and cheap PPL agencies underperform for cash-pay clinics?
Because they optimize for the cheapest possible lead instead of the most ready-to-buy patient.
For a high-ticket cash-pay clinic, those are opposite goals.
A generic e-book or free-guide funnel run by a low-cost pay-per-lead agency collects emails from people who wanted the freebie, not the treatment.
So the leads sit far back in the awareness journey and rarely convert into paid appointments.
The agency reports a low cost per lead and calls it a win.
But cost per lead is a vanity number.
The only metrics that matter for a cash-pay clinic are cost per booked appointment and the lifetime value of the patient who shows up.
A cheap lead that never books is infinitely expensive.
These funnels also tend to be templated and run identically across dozens of unrelated businesses.
So the messaging never matches your treatment, your demographic, or your local market.
Compare that to channels you can actually control and improve:
- Your own SEO
- Your Google Business Profile
- Your owned social brand
With those, you tune the offer, the page, and the follow-up until the economics work.
And the lead chose you on purpose.
What should a cash-pay clinic run instead of these bad lead sources?
Run channels you own and can compound.
Start with SEO and your Google Business Profile.
Then add properly built paid acquisition matched to the treatment.
SEO is the single best way to build sustainable lead flow in a cash-pay clinic.
The leads are the most ready to buy and the most familiar with the business by the time they reach you.
It also compounds for years when paired with strong Google reviews and an established social brand.
Eternity Health Partners built a roughly 1.7 million dollar per year revenue line from SEO as a high-intent channel.
Orthobiologics Associates grew on SEO alone and converts inbound at a 79.4 percent rate.
That is what high-intent, self-selected demand looks like compared to a purchased aggregator list.
From there, match paid channels to the treatment:
- TikTok for aesthetics
- Facebook for joint pain and higher-ticket cash offers run with a real funnel and fast follow-up
- Google and YouTube for product-aware search demand
The principle behind all of it is to own the relationship and control the offer.
Do not rent an audience that never chose you.
Pick channels you can control, improve, and scale.
That is the whole grading rubric.
How do you grade a lead source before you spend money on it?
Grade every lead source on four criteria before you spend a dollar:
- Difficulty
- Scalability
- Quality
- Speed
Difficulty asks whether you can run and improve it yourself.
If you do not control the offer, the audience, the creative, and the funnel, you can never fix it when it underperforms.
That is why aggregators and deal platforms are uncoachable.
Scalability asks whether getting it right means you can pour more in and get more out.
A shared-lead marketplace caps out the moment the pool is exhausted.
SEO and owned paid channels scale with investment.
Quality asks how ready-to-buy the leads are with a good offer.
A patient who searched for your treatment by name and chose your clinic is worlds ahead of a discount-seeker or a name on a resold list.
Speed asks how fast it produces real booked appointments, not how fast it produces raw leads.
Run any channel through those four questions and the worst lead sources eliminate themselves.
They are hard to improve.
They are impossible to scale.
They are low in quality.
And they are only fast at generating noise.