Is a Low Cost-Per-Lead Actually Good for a Cash-Pay Clinic?
If we had a dollar for every doctor who told us they did not care about cost-per-lead — and for every one who chased the cheapest CPL straight off a cliff — we could fund a clinic ourselves.
Both instincts are wrong.
CPL matters, but not the way most clinic owners think.
A low cost-per-lead is not the goal. A low cost-per-acquired-patient is.
The cheapest leads can quietly lose you money. And slightly pricier leads can be the best money you spend all year.
This is the FAQ on what CPL actually means for a cash-pay clinic, how to reverse-engineer the number you can afford, and what to optimize instead of the headline you see in your ad account.
Is a low cost-per-lead always a good thing for a cash-pay clinic?
No — a low cost-per-lead is only good when it produces a low cost-per-acquired-patient.
CPL is an input metric, not an outcome.
The cheapest CPL in your ad account tells you almost nothing on its own.
A lead is just a name and a phone number.
It has not booked.
It has not shown up.
And it has not paid you anything yet.
Cheap leads that never convert cost you more than expensive leads that do.
The wasted sales-team hours, the no-shows, and the lost calendar capacity never appear on the CPL line.
You only see the damage when you carry the cost all the way down the funnel:
- Spend
- Leads
- Booked appointments
- Attended consults
- Closed patients
This is why the right way to think about CPL is to start at the end and reverse-engineer the numbers.
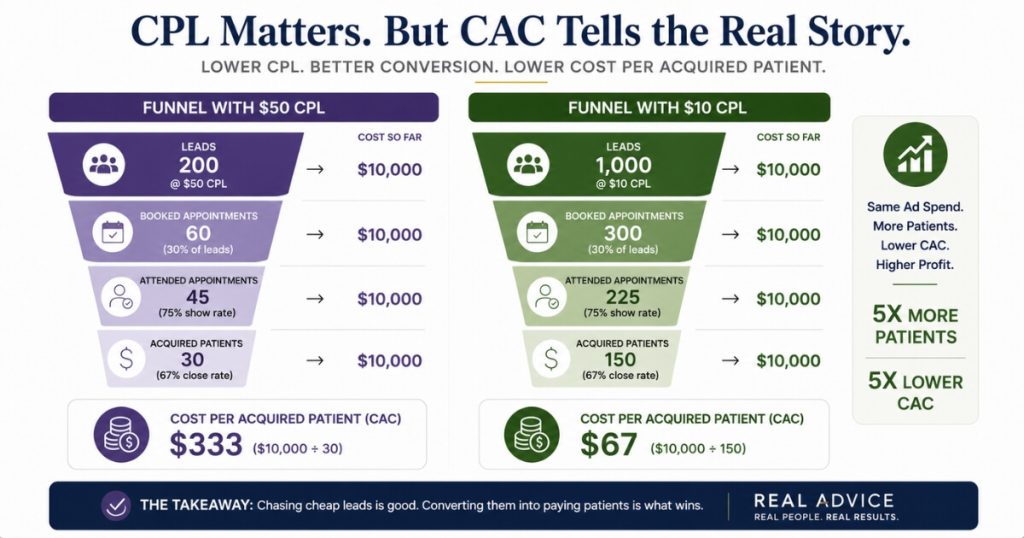
If $10 leads close at half the rate of $50 leads, the $10 leads can still win.
But the only metric that reveals that is cost-per-acquired-patient, not the headline you are tempted to brag about.
The whole discipline of profitable patient acquisition comes down to optimizing the bottom number, not the top one.
What number should a cash-pay clinic optimize instead of cost-per-lead?
Cost to acquire a patient — your CAC — benchmarked against the profit of the program you are selling.
That is the number that decides whether a campaign lives or dies.
Start at the end and work backwards.
If a program is worth $1,000 and your margin is 70%, you make $700 in profit on each new patient.
You need that number first.
It is what justifies how much you can spend to acquire a customer.
To double your money, you need to acquire that patient for under $350.
We would always want a better return on ad spend than two-to-one.
But $350 is the ceiling that keeps you profitable.
And it is a real number from your own books, not a CPL figure a competitor is bragging about.
Once you have the CAC ceiling, every upstream metric becomes a checkpoint, not a target.
That includes:
- Cost per lead
- Cost per booked appointment
- Cost per attended consult
They are all just mile markers on the road to CAC.
Set the ceiling first.
Then back into the CPL the funnel actually requires to hit it.
A clinic that does this stops asking, “Is my CPL low?”
It starts asking, “Does my CPL deliver patients under my CAC ceiling?”
How do you reverse-engineer the cost-per-lead you can actually afford?
You work backwards from your target CAC through every conversion rate in the funnel.
One stage at a time.
Here is the worked example.
You can spend $350 to acquire a patient, and you close 70% of the patients you get in front of at an initial consult.
To stay inside that, you need five attended consults for every $1,000 you spend.
That is $200 per attended consult.
Account for the close rate and you are at roughly $340 of cost per closed new customer.
That is comfortably under the $350 ceiling.
Now climb back up the funnel.
At a 70% show rate, getting five attended consults means booking 8.5 consults.
That puts you at about $117 per booked appointment.
Keep going.
If you book 50% of every lead that comes in, and you need booked appointments at $117, you need leads at roughly $50 each.
Run the whole chain forward to check it:
- $1,000 spent at $50 per lead buys 20 leads.
- Book 50% and you have 10 appointments at $100 each.
- 70% attend and you have 7 attended consults at $142.
- Close 70% and you have 5 new patients at a $200 CAC.
The CPL you can afford — $50 — is an output of the funnel.
It is not a number you pick in advance.
Why can cheap leads lose money even when the cost-per-lead looks great?
Because lead quality changes every downstream conversion rate.
A flattering CPL attached to weak conversion can still blow straight past your CAC ceiling.
Run the same $1,000 model and watch how fragile it is to lead price.
If your math needs leads at $50 to land a $200 CAC, leads at $75 break the model.
Leads at $100 definitely do not work.
That is true even if $100 leads look perfectly reasonable in isolation, especially against a competitor paying $200.
The CPL in isolation is meaningless.
It only means something against the conversion rates that follow it.
The trap is worse than a price mismatch, though.
Low-quality leads are not just cheap.
They typically book, show, and close at lower rates than qualified leads.
So the real cost-per-acquired-patient balloons at the exact moment the CPL line is dropping and looking its best.
A clinic owner staring at a falling CPL feels like they are winning.
Meanwhile, CAC quietly climbs out of profitable range.
The CPL line hides the damage.
The CAC line is the only one that exposes it.
Are there cases where a genuinely low cost-per-lead is a home run?
Yes — when the leads are genuinely cheap and you have a nurture system in place to raise their quality.
That combination is where a low CPL turns into a windfall.
If your model already works at $50 leads and you suddenly start getting leads at $10, that is a home run.
Why?
Because you can implement:
- Nurture systems
- Fast speed-to-lead
- Tighter qualification
Those systems make the leads more engaged and higher quality.
At $10 per lead, $1,000 buys 100 leads instead of 20.
Even if the cheaper traffic converts at a lower rate, the sheer volume plus a real follow-up operation can drive cost-per-acquired-patient down dramatically.
The proof is in the funnel.
At the same spend, lower CPL with intact conversion simply produces more patients per dollar.
But notice the condition.
The win is never the cheap CPL by itself.
It is cheap leads plus the operational machine that converts them.
Cheap leads with no nurture, no speed-to-lead, and no qualification are just cheap waste.
The clinics that turn a $10 CPL into a flood of patients are the ones that already had the systems built before the cheap leads arrived.
How does lead-to-booked conversion change the cost-per-lead math?
Dramatically.
Your booking rate is the single biggest multiplier on what you can afford to pay per lead.
That means improving conversion beats chasing a cheaper CPL almost every time.
Look back at the worked example.
It assumed you book 50% of your leads.
That one assumption is doing enormous work.
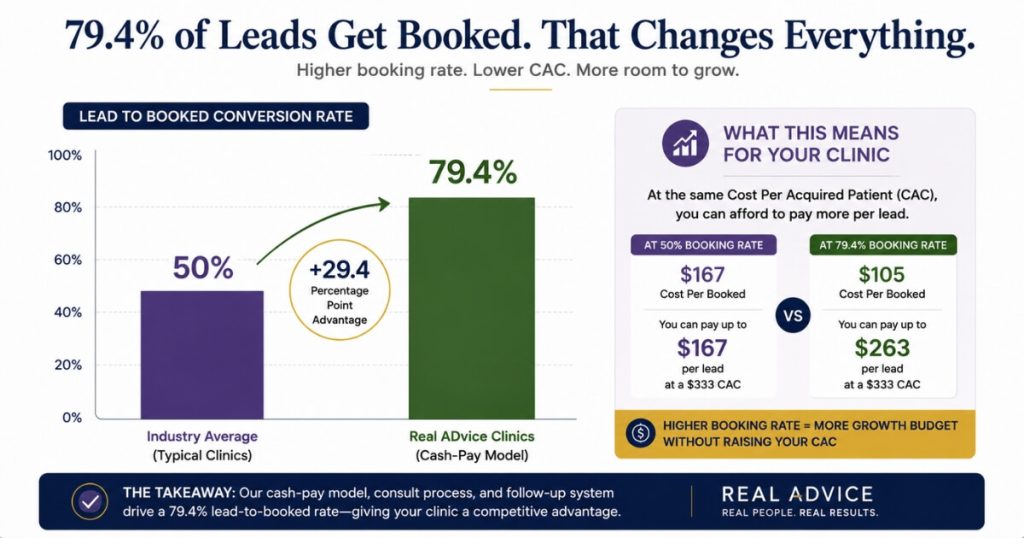
A clinic that converts leads to booked appointments at nearly 80% can pay far more per lead and still hit the same CAC.
Why?
Because each lead is worth so much more on the way down the funnel.
We took a regenerative-medicine clinic to a 79.4% lead-to-booked conversion rate, which means roughly the same ad spend produced far more booked consults than a clinic booking only half its leads.
This is why “fix the booking rate before you fixate on CPL” is the right order of operations.
Higher conversion lets you outbid competitors on leads while keeping your CAC lower than theirs.
That is the exact opposite of the race-to-the-cheapest-lead strategy.
The same discipline shows up on the paid side.
A dialed-in offer, ad team, and follow-up engine is how we added $2M in revenue from Facebook ads alone at an orthopedic surgical practice.
They did not win by buying the cheapest leads.
They won by converting the leads they bought.
FAQ’s About Whether Low CPL Is Good
Is a low cost-per-lead always a good thing for a cash-pay clinic?
No — a low cost-per-lead is only good when it produces a low cost-per-acquired-patient.
CPL is an input metric, not an outcome.
Cheap leads that never book, never show, or never close cost you more than expensive leads that convert.
Why?
Because the wasted sales-team hours and lost capacity do not show up in the CPL line.
The honest test is to carry the cost all the way down the funnel:
- Spend
- Leads
- Booked appointments
- Attended consults
- Closed patients
If $10 leads close at half the rate of $50 leads, the $10 leads can still win.
But only the cost-per-acquired-patient tells you that.
The headline CPL does not.
Optimize the bottom number, not the top one.
What number should a cash-pay clinic optimize instead of cost-per-lead?
Cost to acquire a patient, or CAC, benchmarked against the profit of the program you are selling.
Start at the end.
If a program is worth $1,000 at a 70% margin, you profit $700.
That means you can spend up to $350 to acquire a patient and still double your money.
That $350 ceiling is the number that decides whether a campaign works.
Not a CPL target your competitor brags about.
Every upstream metric is just a checkpoint on the way to CAC.
That includes:
- CPL
- Cost per booked appointment
- Cost per attended consult
Set the CAC ceiling first.
Then back into the CPL the funnel actually requires.
How do you reverse-engineer the cost-per-lead you can actually afford?
Work backwards from your target CAC through every conversion rate in the funnel.
Say you can spend $350 to acquire a patient and you close 70% of attended consults.
You need five attended consults per $1,000 spent.
That is $200 per attended consult.
At a 70% show rate, you need 8.5 booked consults.
That is about $117 per booked appointment.
If you book 50% of leads, you need leads at roughly $50 each.
So with $1,000, you buy 20 leads at $50.
You book 10.
Seven attend.
And you close five at a $200 CAC.
The CPL you can afford is an output of the funnel math.
It is not a number you pick in advance.
Why can cheap leads lose money even when the cost-per-lead looks great?
Because lead quality changes every downstream conversion rate.
A great CPL attached to bad conversion can still blow past your CAC ceiling.
If your model needs leads at $50 to hit a $200 CAC, leads at $75 break the math.
Leads at $100 lose money outright.
That is true even if $100 leads look fine in isolation against a competitor paying $200.
Worse, low-quality cheap leads usually book, show, and close at lower rates.
So the real cost-per-acquired-patient balloons even as the CPL drops.
The CPL line hides the damage.
The CAC line exposes it.
Are there cases where a genuinely low cost-per-lead is a home run?
Yes — when the leads are cheap and you have a nurture system to raise their quality.
If your model works at $50 leads and you suddenly get leads at $10, that is a home run.
Why?
Because you can layer nurture, speed-to-lead, and qualification on top.
At $10 per lead, $1,000 buys 100 leads instead of 20.
Even at lower conversion rates, the cost-per-acquired-patient can fall dramatically.
But the win is not the cheap CPL by itself.
It is cheap leads plus the operational system that converts them.
Cheap leads with no follow-up are just cheap waste.
How does lead-to-booked conversion change the cost-per-lead math?
Dramatically.
Booking rate is the single biggest multiplier on what you can afford to pay per lead.
Most of the funnel math assumes a 50% booking rate.
But a clinic that converts leads to booked appointments at nearly 80% can pay far more per lead and still hit the same CAC.
We took one regenerative-medicine clinic to a 79.4% lead-to-booked conversion rate.
That means roughly the same ad spend produced far more booked consults than a clinic booking half its leads.
Fix the booking rate before you fixate on CPL.
Improving conversion lets you outbid competitors on leads while keeping CAC lower than theirs.