How Do You Get Patients to Say Yes to an Unfamiliar Regenerative Procedure?
Selling a regenerative procedure patients already know — like a knee injection they have read about — is hard enough.
Selling one they have never heard of, like percutaneous tenotomy or prolotherapy, is a different problem entirely.
The patient cannot Google a name they cannot spell. They cannot compare it to anything. They cannot explain it to their spouse.
So they default to the safest thing a nervous person can do: nothing.
This is the playbook for turning that nothing into a yes — not with a harder pitch, but with patient education, careful framing against surgery, and proof delivered in low-pressure doses over time.
It is built from the nurture sequences that actually convert cash-pay regenerative consultations.
Why won’t patients book a regenerative procedure they have never heard of?
Because an unfamiliar name triggers risk, not curiosity — and risk freezes the decision.
When a patient hears a term like percutaneous tenotomy or prolotherapy for the first time, they have no mental file for it.
They cannot compare it to anything they already understand.
In addition, they cannot picture the outcome.
They cannot tell a friend what they are about to do.
That uncertainty reads as danger.
And when a healthcare decision feels dangerous, the safest move — the one the brain defaults to — is to wait.
Not say no, just wait.
Which is functionally the same thing for your calendar.
The mistake most clinics make is responding to this hesitation with volume:
- A bigger discount
- A harder phone call
- A more aggressive landing page
That increases the perceived risk, because pressure is what salespeople apply and trust is what doctors earn.
The fix is the opposite.
You move a problem-aware person — someone who already raised their hand by requesting information — toward a decision they can defend to themselves and to their family.
You do it with education delivered in small, repeated doses.
That way, the procedure stops feeling foreign and starts feeling like the obvious next step.
That is why the first message in a high-converting sequence almost never names the procedure at all.
It simply thanks the patient for taking the first step toward getting out of pain and invites their questions.
How do you build trust before you ever ask a patient to commit?
You lead with their problem and your credibility, and you let the procedure come later.
Trust in healthcare is built on three things a patient can feel before they ever sit in your chair:
- That you understand their pain
- That other people like them got better
- That you are not going to pressure them
A nurture sequence that respects this opens by thanking the patient for reaching out and opening the door to questions.
It does not open by naming the treatment.
The job of the first touch is purely to lower the patient’s guard and confirm they made a good decision by contacting you.
The second touch finds common ground.
You both want the same outcome — the patient’s health — and you make that explicit.
Then you list the conditions you actually treat:
- Peripheral neuropathy
- Fibromyalgia
- Tendonitis
- Migraines
- Neck and back pain
- Osteoarthritis
- Sports injuries
This list does quiet, powerful work.
It lets the patient recognize themselves on the page.
The moment a reader thinks “that’s my elbow” or “that’s my mother’s neuropathy,” they have stopped being a passive recipient and started being a candidate.
Only after a patient has identified with a condition and felt understood do you introduce the new service by name.
By then, you are not introducing a stranger.
You are answering a question they have already begun asking.
For clinics that want this same compounding trust at scale through search and reviews rather than only email, our stem cell clinic marketing approach builds the same credibility signals across every channel a regenerative patient touches.
How should you introduce a procedure like percutaneous tenotomy by name?
Introduce it as news, not as a pitch.
Frame it as the newest thing you offer and let your existing patients do the convincing.
The most effective way to name an unfamiliar procedure is to position it as a recent addition you are genuinely excited about.
Then link to a plain-language explanation the curious can read on their own.
Immediately attach social proof: our patients won’t stop raving about it.
That one move does three jobs at once:
- It signals the treatment is current and backed by the latest technology and studies.
- It transfers credibility from people who already trust you to a person who does not yet.
- It keeps the stakes low by framing the next step as a free consultation to learn more.
Naming matters because an unnamed procedure cannot be researched.
And a researched procedure feels safer.
So name it once you have earned the right to.
Link out so the self-directed patient can educate themselves.
Let the rave reviews carry the emotional weight that a clinical description never can.
The patient does not need to fully understand percutaneous tenotomy to book a consultation.
They need to feel that real people, with problems like theirs, are glad they did it.
And they need to feel that the only thing being asked of them right now is a conversation.
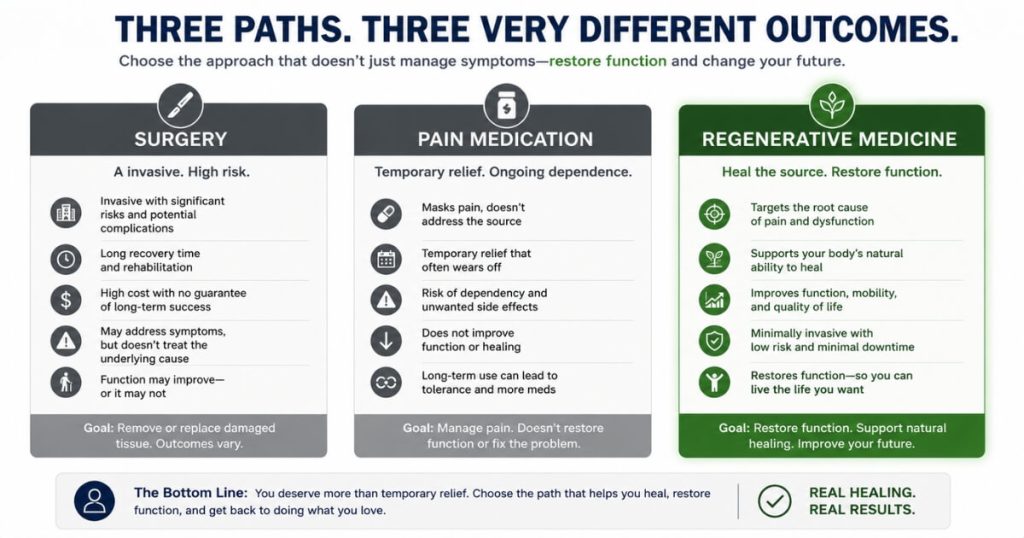
How do you frame a regenerative procedure against surgery or pain medication?
Frame it as the option that restores function instead of masking pain or cutting into the body — and let a real patient say the word surgery for you.
Patients weighing a regenerative procedure are almost always comparing it, silently, to two things they already understand:
- Surgery
- Long-term pain medication
Both carry baggage.
Surgery means downtime, scarring, anesthesia, and real risk.
Pain medication means dependence, side effects, and a problem that is managed but never actually solved.
Regenerative medicine wins this comparison when you describe it the way it actually works.
It restores the structure and function back to damaged cells and tissues rather than masking symptoms.
The contrast is stronger when it is voiced by a patient instead of by you.
This is where testimonials become the most persuasive asset you own.
A line like “I am so happy I chose to not get surgery on my knee — Dr. did several regenerative treatments and I am good as new” does more than any clinical chart.
It gives the prospect two things they cannot get anywhere else:
- Permission to want the less invasive path
- A real person to identify with
Another patient noting that the doctor “does not use pain meds to mask the pain — he really looks at the problem” closes the second comparison.
Your job is to make the comparison the patient is already running explicit.
Then resolve it with proof.
You do not have to attack surgery.
You only have to let a patient who chose the alternative be heard.
What does a patient-education email sequence for a new regenerative service look like?
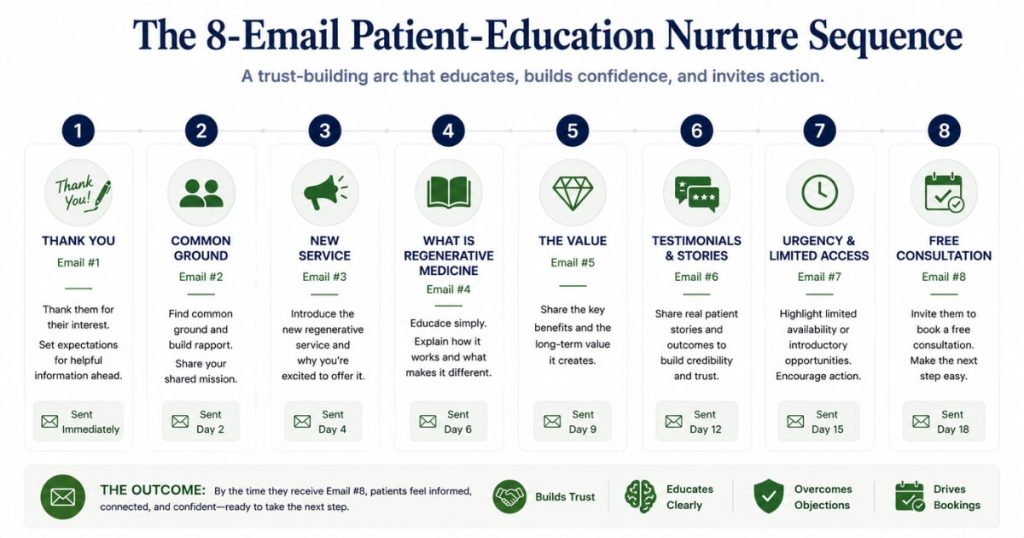
It is a multi-touch arc that moves from gratitude to identification to the new service to proof to urgency.
Roughly eight emails, each with one job and one soft call to action.
A sequence that converts unfamiliar regenerative procedures does not try to do everything in one message.
Each email carries a single job.
- Email one thanks the patient and opens the door to questions.
- Email two finds common ground and lists the conditions you treat so the reader self-identifies.
- Email three introduces the new service by name as exciting news, with a link and social proof.
- Email four explains the broader category — what regenerative medicine actually is and what falls under it.
That includes:
- Prolotherapy
- PRP injections
- Stem cell therapy
- Percutaneous tenotomy
Email five adds pure value with no ask, such as how diet and specific supplements make treatment more effective.
This is the email that turns you from a vendor into a teacher.
From there, the sequence shifts toward decision.
- Email six is pure social proof — named patient testimonials and video reviews.
- Email seven creates gentle urgency around the free consultation offer.
- Email eight paints the after picture: imagine living pain free and loving every minute of it.
The connective tissue across all eight is one consistent, low-friction call to action:
Book your free consultation now.
That way, the patient can act the instant their readiness crosses their hesitation, rather than waiting for you to call.
The clinics that pair this kind of nurture with strong search and review presence see the compounding effect directly.
Orthobiologics Associates generated $309,590 in cash-pay revenue from SEO at a 79.4% conversion rate, because the patients arriving were already educated and already trusting before the consultation began.
How do you handle the objection that the patient wants to think about it?
You give them more reasons to feel safe instead of more pressure to decide.
And you keep the free consultation the only thing you ever ask for.
“I want to think about it” is rarely about thinking.
It is unresolved fear or an unanswered question wearing a polite disguise.
The clinics that convert these patients do not chase them.
They nurture them.
They keep delivering value and proof on a schedule:
- A testimonial here
- A teaching email there
- A quiet reminder that the consultation is free and carries no obligation
The consultation itself is the pressure-release valve.
It is framed as a conversation to learn which route is most suitable for the patient’s situation.
It is not framed as a sales appointment with a contract at the end.
When the only commitment you ever request is a free, low-stakes conversation, the patient’s natural caution stops working against you.
It starts working for you.
Saying yes to a conversation feels safe.
The patient who needs eight weeks gets eight weeks of gentle, valuable contact.
Then they book when the desire to be out of pain finally outweighs the fear.
This is the same dynamic that lets dialed-in regenerative practices scale dramatically once the education engine is running.
Elite Pain Doctors produced $2,095,039 in 10 months by combining trust-first patient education with a system that captures and nurtures every problem-aware lead until they are ready.
FAQ’s About Getting Patients to Try New Regenerative Procedures
Why won’t patients book a regenerative procedure they have never heard of?
Because an unfamiliar name triggers risk, not curiosity — and risk freezes the decision.
When a patient hears a term like percutaneous tenotomy or prolotherapy for the first time, they have no mental file for it.
They cannot compare it to anything.
Also, they cannot picture the outcome.
They cannot tell a friend what they are about to do.
That uncertainty reads as danger.
The safest thing a nervous patient can do is nothing.
The fix is not a louder pitch.
It is education delivered in small, low-pressure doses over time.
That way, the procedure stops feeling foreign and starts feeling like the obvious next step.
You are not selling a procedure to a stranger.
You are moving a problem-aware person who already raised their hand toward a decision they can defend to themselves and to their spouse.
That is why the clinics that win these cases do it with a nurture sequence, not a single appointment.
It is also why the first message in that sequence almost never mentions the procedure at all.
It thanks the patient for taking the first step toward getting out of pain.
How do you build trust before you ever ask a patient to commit?
You lead with their problem and your credibility, and you let the procedure come later.
Trust in healthcare is built on three things a patient can feel before they ever sit in your chair:
- That you understand their pain
- That other people like them got better
- That you are not going to pressure them
A good email or nurture sequence opens by thanking them for taking the first step toward getting out of pain and inviting questions.
It does not open by naming the treatment.
The second touch finds common ground.
You both want the same outcome: their health.
Then you list the conditions you actually treat:
- Peripheral neuropathy
- Fibromyalgia
- Tendonitis
- Migraines
- Neck and back pain
- Osteoarthritis
- Sports injuries
That lets them recognize themselves on the page.
Only after the patient has identified with a condition and felt understood do you introduce the new service by name.
By then, you are not introducing a stranger.
You are answering a question they have already started asking.
How should you introduce a procedure like percutaneous tenotomy by name?
Introduce it as news, not as a pitch.
Frame it as the newest thing you offer and let your existing patients do the convincing.
The most effective way to name an unfamiliar procedure is to position it as a recent addition you are excited about.
Then link to a plain-language explanation and immediately attach social proof: patients will not stop raving about it.
That single move does three things at once:
- It signals that the treatment is current and backed by the latest technology and studies.
- It transfers credibility from people who already trust you to people who do not yet.
- It lowers the stakes by framing the next step as a free consultation to learn more.
Name the procedure once you have earned the right to.
Link out so the curious can self-educate.
Let the rave reviews carry the emotional weight that a clinical description never can.
How do you frame a regenerative procedure against surgery or pain medication?
Frame it as the option that restores function instead of masking pain or cutting into the body.
Then let a real patient say the word surgery for you.
Patients weighing a regenerative procedure are almost always comparing it, silently, to two things they already understand:
- Surgery
- Long-term pain medication
Both carry baggage.
Surgery means downtime, scarring, and risk.
Pain meds mean dependence and a problem that never actually goes away.
Regenerative medicine wins this comparison when you describe it as restoring the structure and function back to damaged cells and tissues rather than masking symptoms.
The contrast becomes stronger when it comes from a patient’s mouth, not yours.
A testimonial like “I am so happy I chose to not get surgery on my knee” does more than any chart.
It gives the prospect permission to want the less invasive path and a real person to identify with.
Make the comparison the patient is already making explicit.
Then resolve it with proof.
What does a patient-education email sequence for a new regenerative service look like?
It is a multi-touch arc that moves from gratitude to identification to the new service to proof to urgency.
Roughly eight emails, each with one job and one soft call to action.
A proven structure runs like this:
- Email one: Thank them and open the door to questions.
- Email two: Find common ground and list the conditions you treat so they self-identify.
- Email three: Introduce the new service by name as exciting news.
- Email four: Explain the broader category — what regenerative medicine actually is and which services fall under it.
- Email five: Add value with no ask, such as how diet and supplements make treatment more effective.
- Email six: Share pure social proof — named patient testimonials and video reviews.
- Email seven: Create gentle urgency around the free consultation offer.
- Email eight: Paint the after picture: imagine living pain free.
Every email carries the same low-friction call to action:
Book your free consultation now.
That way, the patient can act the moment they are ready, not when you happen to call.
How do you handle the objection that the patient wants to think about it?
You give them more reasons to feel safe instead of more pressure to decide.
And you keep the free consultation the only thing you ever ask for.
“I want to think about it” is rarely about thinking.
It is unresolved fear or unanswered questions.
The clinics that convert these patients do not chase.
They nurture.
They keep delivering value and proof on a schedule:
- A testimonial here
- A teaching email there
- A reminder that the consultation is free and carries no obligation
The consultation itself is the pressure-release valve.
It is framed as a conversation to learn which route is most suitable for the patient’s situation.
It is not framed as a sales appointment.
When the only commitment you ever request is a free, low-stakes conversation, the patient’s natural caution stops working against you.
The patient who needs eight weeks gets eight weeks of gentle, valuable contact.
Then they book when the fear finally falls below the desire to be out of pain.