How Do You Build a Cash-Pay Telehealth Funnel That Doesn’t Lose Leads?
Most cash-pay telehealth clinics do not have a traffic problem.
They have a leak problem.
The leads are coming in — forms, texts, self-scheduled consults — and then they quietly disappear in the gaps.
The gap between the website and the calendar.
While the gap between the front desk and the provider.
The gap between the moment a patient raises a hand and the moment a human responds.
In one month at a single telehealth practice, we counted 74 cash leads and could only confirm what happened to 16.
This is the field guide to plugging that leak: one booking system, true speed-to-lead, a card-on-file deposit that kills no-shows, a price-shopper script that converts, and a recovery audit for the leads already lost.
What does it actually mean for a cash-pay telehealth funnel to “lose” a lead?
A lost lead is any cash-pay prospect who raised a hand — filled out a form, texted, or self-scheduled — and never got serviced or charged because the funnel dropped them somewhere along the way.
It almost never looks like a dramatic failure.
It looks like a patient who self-scheduled a discovery call and was never called because the booking landed somewhere the provider does not check.
Also, it looks like a lead silently dragged to “no longer interested” with not a single message attached.
It looks like a patient texting “I can’t even get an appointment” right before they walk away.
Those are not edge cases.
In one tracked month, of 74 cash leads, only 16 self-scheduled inside the system the team could actually monitor.
The reason this matters for cash-pay is the unit economics.
You paid to acquire every one of those leads.
And a telehealth weight-loss, peptide, or HRT patient is high-margin and often recurring.
So a single lost lead is the lifetime value of a paying patient evaporating because of an operational gap.
Lead loss in telehealth is a patient-acquisition problem disguised as a marketing problem.
The first step to fixing it is admitting the leads are already there.
Why do telehealth leads leak before they ever pay?
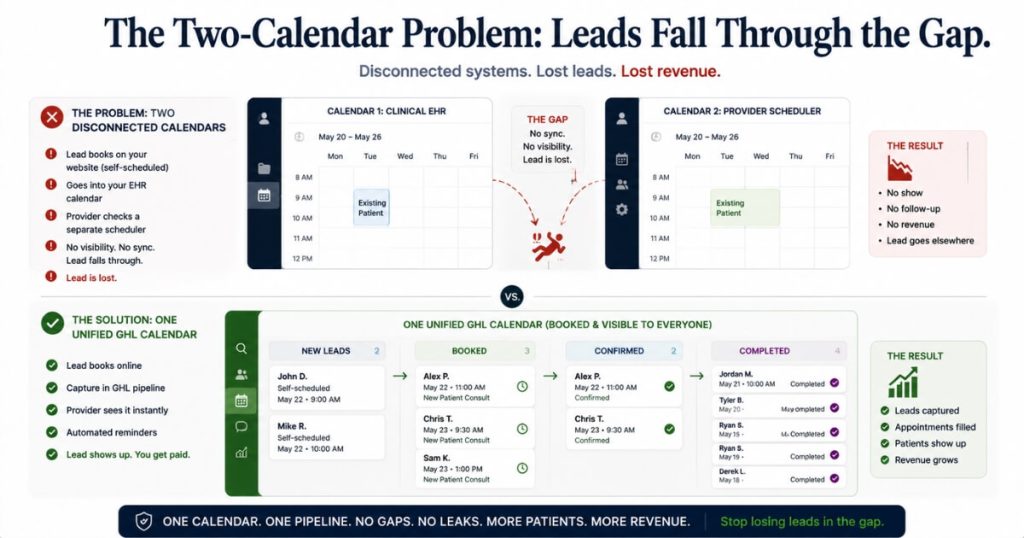
They leak because the booking lives in two places, the follow-up lives in a third, and nobody owns the gap in between.
The single biggest leak is the two-calendar problem.
The front desk books cash-pay consults in the clinical EHR because that is where charting happens.
The provider works from a separate calendar.
Self-scheduled website leads land in a CRM neither of them watches closely.
A patient books a 3pm telehealth consult on the website.
It never appears on the provider’s calendar.
The provider never calls.
The patient texts “why did no one call me?”
And now you have a dead lead, even though every system did exactly what it was built to do.
The team cannot even tell what happened without opening each lead one at a time.
That is because the outcome was never recorded in a shared place.
The second leak is speed.
A telehealth buyer behaves like someone trying to find a doctor they can talk to today.
So when one texts “do you have an opening today at 3pm?” and hears back tomorrow afternoon, they are already gone.
The third leak is tone.
A cold, automated reply like “we have an appointment at 3, do you want it?” makes the prospect feel like a number.
And a prospect who feels like a number does not hand over a credit card.
None of these are creative or budget failures.
They are operational leaks between capture and payment.
Every one is fixable with a single system and a repeatable process.
What is the single most important fix for a leaky cash-pay telehealth funnel?
Put every cash-pay lead, booking, call, and outcome into one system so nothing can hide.
When the front desk books in the EHR and the provider works from a separate scheduler, leads fall through the crack between them.
No one can see outcomes without manual archaeology.
The fix is to make a single CRM — for our clients that is GoHighLevel (GHL) — the one and only place cash-pay consults are booked.
It is also where the provider makes outbound calls and every disposition is recorded.
The rule we give every clinic is blunt:
If it is cash-pay, it gets booked here and only here.
Insurance patients can stay in the clinical system.
The cash-pay telehealth schedule lives in one shared calendar.
One system does three things at once.
First, booking through a single calendar link automatically moves the lead into the booked-appointment stage.
That means the provider never checks two places and self-scheduled leads stop vanishing.
Second, when the provider calls through the CRM, the team can listen to the recording, coach the close, and see the result in real time.
Third, every lead carries a visible disposition:
- Booked
- Attended
- No-show
- Not interested
That makes the whole pipeline legible at a glance.
Most of the leakage stops the day the second system is switched off.
This is the operational backbone of the broader patient acquisition system for cash-pay clinics, because the best ads cannot outrun a funnel that drops the leads they generate.
How fast do you have to respond to a telehealth lead?
Respond within minutes.
And engineer it so a human is staring at a list of unbooked leads every single day, rather than waiting for an alert to maybe appear.
Because telehealth buyers want care today, speed-to-lead is decisive.
But “respond fast” is useless unless someone owns a specific list every day.
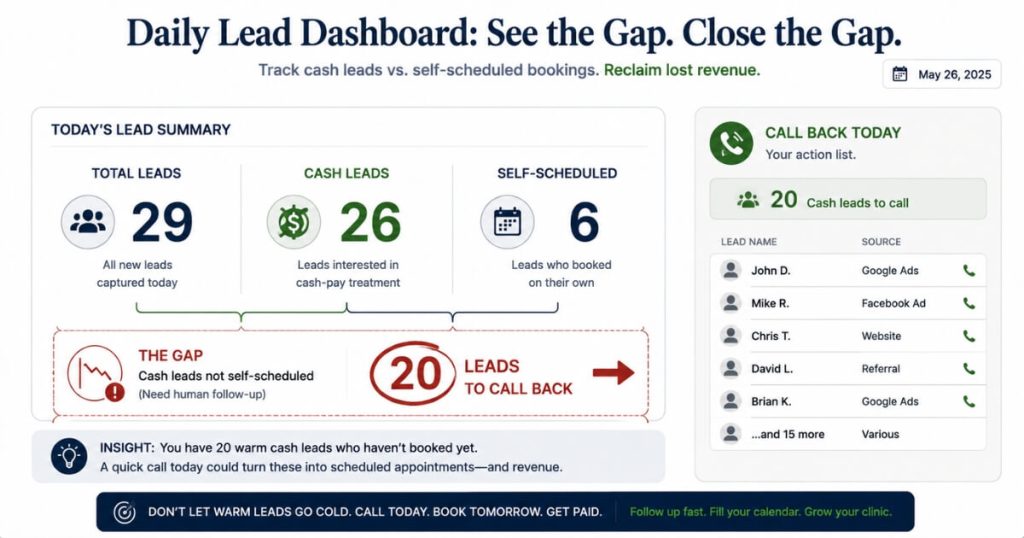
The mechanism that makes it real is a dashboard checked daily showing:
- Total leads
- Cash leads
- How many of those actually self-scheduled
The gap between those numbers is your leak, in plain numerals.
In one recent week, a clinic had 29 total leads.
26 of them were cash.
Only 6 self-scheduled.
That is a 20-lead gap sitting there waiting to be called.
The workflow that closes it is simple and repeatable.
Open the dashboard every morning.
Click the gap to open the list of unbooked cash leads.
Work down it from a single screen, placing each outbound call through the CRM so it is logged and coachable.
Then drag each contact into its next stage as you go.
Speed-to-lead is not a personality trait.
It is a list with an owner who clears it daily.
Clinics that install this rhythm see the pattern that drove a 900% lead increase and 100+ calls per month at VYVE Wellness.
The volume was always achievable once the follow-up stopped leaking.
How does a deposit or card-on-file stop leads from leaking and cut no-shows?
Collecting a card to reserve the slot — even for a free consult — filters out tire-kickers and gives the no-show a real cost, without adding a price barrier to booking.
Many cash-pay clinics move to a free consult to remove every barrier to entry.
That is the right call for volume.
But a free consult with zero commitment is an open invitation to no-show.
And a calendar full of no-shows is just lead loss wearing a costume.
The resolution is to keep the consult genuinely free while still capturing a card on file tied to a no-show fee.
Frame it so it never feels like a charge:
“All of our consults are free — there’s absolutely no charge to you. We just request a card on file to reserve the slot. Your card will never be charged unless you no-show or cancel within 24 hours.”
That one line does the work of three.
It screens for serious buyers without scaring off the curious.
It drops the no-show rate because the appointment now has a cost attached.
And it puts a card in the patient’s profile before the consult even happens, which makes the eventual close far smoother.
The leak to watch is consistency.
The deposit only works if the card is collected on every booking.
That includes the consults the front desk schedules manually by phone, not just the self-scheduled ones.
Enforce it half the time and you get the worst of both worlds.
What do you say to a price-shopper so the lead converts instead of leaking?
Stop treating price-shoppers as tire-kickers and lead with a single question:
“Have you tried this before, or would this be your first time?”
Price-shopping is normal.
Everybody wants to know what something costs.
A prospect asking about price is not unmotivated.
They simply lack information and value.
The reply that leaks these leads is the cold, canned line “we can schedule this if you want.”
That reads as automated and makes the person feel like a number.
The reply that converts opens a real conversation.
When someone asks about a service, the go-to response is always:
“Great, happy to help. Have you tried weight-loss injections before, or would this be your first time?”
Swap in peptides or HRT or whatever they asked about.
That question surfaces their history.
Most people exploring a GLP-1 have tried something else.
It gets them talking about their actual goal and earns you the right to walk them toward a booking.
On price, give an honest range:
“The starting dose is roughly this, and some patients on higher doses invest around that.”
Then route them into the free provider consult to finalize.
We have watched a provider with a genuine 70% close rate still leave money on the table purely because leads leaked before they ever reached him.
Fix the funnel and a strong close rate compounds instead of getting starved.
It is the same dynamic behind the steady inbound flow at Eternity Health Partners, which runs 60 inbound calls and 40 website leads a month.
How do you recover the cash-pay leads that already slipped through the cracks?
Run a backlog audit.
Pull every self-scheduled and booked cash-pay lead from the last 30 days.
Find the ones with no outcome recorded.
Then call them back.
Most clinics never do this for one reason:
Without a single system, there is no way to see outcomes at scale, so the backlog stays invisible.
Once everything lives in one CRM, the audit becomes mechanical.
Filter the booked-appointment stage by date range.
Start at the first of last month.
Then filter by your cash-pay tag.
The truth appears:
- Which leads attended
- Which no-showed
- Which got dragged to “no longer interested” with no conversation attached
- Which were simply missed
Each is a recovery opportunity, not a dead end.
Then you work them with empathy instead of a form letter.
That includes the patient who self-scheduled and was never called.
The one who asked a question and got ignored.
The one whose appointment got pushed back and then no-showed.
A surprising number will rebook the moment a real human reaches out and treats them like a patient rather than a line item.
The audit is a one-time cleanup.
The daily dashboard, the single-system discipline, the card-on-file, and the price-shopper script are what stop the backlog from ever rebuilding.
Recovery proves how much revenue was hiding in the leaks.
The system is what keeps it from leaking again.
FAQ’s About Cash-Pay Telehealth Funnels and Lead Loss
How many cash-pay telehealth leads do clinics typically lose?
Far more than they realize.
In one tracked month, a clinic had 74 cash leads and could only confirm what happened to the 16 that self-scheduled in the system everyone could see.
In a single recent week, another snapshot showed 26 cash leads with only 6 self-scheduled.
That is a 20-lead gap.
The leads exist.
They are leaking between systems and between the front desk and the provider.
They are not failing to arrive.
Should the cash-pay consult be free or paid?
Free, but with a card on file.
A free consult removes the barrier to entry and drives volume.
A card-on-file tied to a no-show fee keeps the booking serious.
You get the volume of “free” and the commitment of “paid.”
And the patient has already handed over a card before the consult, which makes the close easier.
What CRM should a cash-pay telehealth clinic use to stop losing leads?
Any single CRM that becomes the one and only place cash-pay leads are booked, called, and dispositioned.
We use GoHighLevel.
The specific tool matters less than the discipline:
- One system
- One calendar link
- All outbound calls logged inside it
- Every outcome recorded there
The leakage comes from running two systems, not from picking the wrong one.
How quickly should we respond to a new telehealth lead?
Within minutes.
Telehealth buyers act like people looking for a doctor they can talk to today.
So a same-day text answered the next afternoon is usually a lost lead.
The reliable way to make that happen is a daily-checked dashboard showing the gap between leads and bookings.
Then one person is responsible for clearing the unbooked list every day.
What is the best opening line for a price-shopping telehealth lead?
“Have you tried this before, or would this be your first time?”
It reframes the price-shopper as someone who simply lacks information.
It opens a real conversation, surfaces their goal, and earns the right to walk them into the free consult.
Give an honest price range when asked.
Then route them to the provider.
Never reply with a cold, canned booking line.