When Should a Cash-Pay Clinic Pause, Fix, or Relaunch Underperforming Google or TikTok Ads?
Most cash-pay clinics react to an underperforming ad campaign in exactly the wrong way.
They cut the budget on a winner because one conversion felt like a fluke, rebuild a whole campaign when the only thing broken was a booking form, or blame the creative when nobody called the leads back.
Pause, fix, and relaunch are three different decisions with three different triggers.
Knowing which one you are looking at is the difference between scaling a profitable channel and quietly burning your monthly budget.
This is the decision framework, pulled from how we diagnose and rebuild Google and TikTok campaigns for cash-pay medical practices.
How long should a cash-pay clinic give a new Google or TikTok campaign before judging it?
Give it enough spend to gather statistically meaningful data, not a fixed number of days.
That means budgeting a floor, not a ceiling.
The rule we use is simple:
Do not spend less than about $20 a day on a new campaign.
Below that, the platform never gathers enough data to optimize.
You are just slowly burning money to learn nothing.
At roughly a $20 cost-per-lead assumption, $20 a day is about $600 a month.
That is enough to collect real signal on whether the campaign produces leads.
When a clinic tells us it wants to relaunch Google on a limited budget, this floor is the first number we set.
Three dollars a day, hoping, is the most common way clinics convince themselves a channel does not work when they never actually tested it.
The first thing a new campaign tells you is volume.
In other words:
Can it produce leads at all?
That answer usually arrives inside the first one to two weeks of consistent spend.
Bookings and paying patients are a separate, slower question.
They depend on:
- Your follow-up
- Your sales process
- Your offer
not just the ad.
So the honest timeline is:
- 1 to 2 weeks to know if the campaign generates leads
- Another 2 to 4 weeks to know if those leads convert
Do not judge a campaign on day three.
Do not cut budget on a campaign producing cheap leads just because nobody has booked yet.
That booking problem almost always lives downstream of the ad.
If you are still deciding which channel deserves the budget, our guide to medical practice marketing maps which treatments convert on which platform.
What signals tell a clinic to pause a campaign versus fix it versus fully relaunch it?
Pause when the platform itself is broken or the spend is producing nothing.
Fix when leads are coming in but not converting.
Relaunch when the underlying offer, landing page, or campaign structure is wrong at the foundation.
Pause
A pause is a delivery problem.
Examples include:
- Your account hit a budget cap
- Ad delivery stalled
- The platform flagged your account for verification
- Leads dropped to zero overnight while spend kept running
We have watched a TikTok account producing eight to eleven leads a day suddenly go to zero in a single day because spend blew through an account-level budget cap in the morning.
That is not a creative or audience failure.
It is mechanical.
You pause, fix the plumbing, and resume the exact same campaign.
Pausing here is maintenance, not a verdict on the ad.
Fix
A fix is a conversion problem.
Leads are arriving at a reasonable cost.
People are answering the phone.
But nobody is booking.
That points downstream, usually to:
- Follow-up speed
- The sales script
- The offer
It does not automatically point to the ad creative.
Relaunch
A full relaunch is a foundation problem.
Examples include:
- The landing page is wrong
- The booking form is broken
- The offer does not match the channel
- The campaign was built around the wrong objective
When you have to swap the landing page, rebuild the booking form, and restructure the campaign before you can even run it again, that is a relaunch.
It is not a tweak.
The mistake clinics make is relaunching when they should fix, and pausing when they should scale.
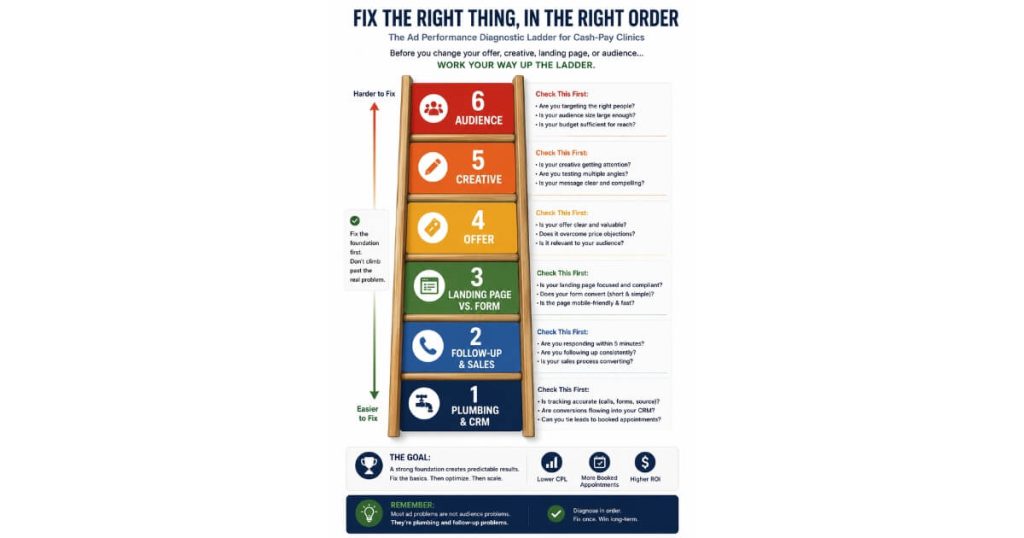
What should a cash-pay clinic change first when ads underperform — offer, creative, landing page, or audience?
Fix the plumbing and the follow-up first.
Do that before you touch the offer, creative, or audience.
Most underperforming clinic campaigns lose money downstream of the ad, not in it.
Start with the mechanical layer.
Confirm that:
- The booking calendar is embedded correctly
- Lead notifications actually reach your sales rep
- The CRM is capturing leads instead of dropping them
- No broken automation is silently killing the funnel
We once found a clinic whose leads were all opting out of texts because the word “stop” had accidentally been baked into the outbound message.
Patients were literally replying “stop” all day and removing themselves from follow-up.
The ads were fine.
The back end was broken.
We have also seen leads pile up uncontacted because the TikTok-to-CRM integration was never connected.
Plumbing first, always.
Second comes follow-up speed and the sales process.
Cash-pay leads need fast contact.
The cash needs to come in as fast as you are putting it out.
A lead that sits for a day is usually a dead lead.
Only after the plumbing and follow-up are clean should you change the funnel itself.
Change things in this order:
- Landing page versus instant form
- Offer
- Creative
- Audience
Change one variable at a time.
Clinics that scramble all four at once can never tell which change worked.
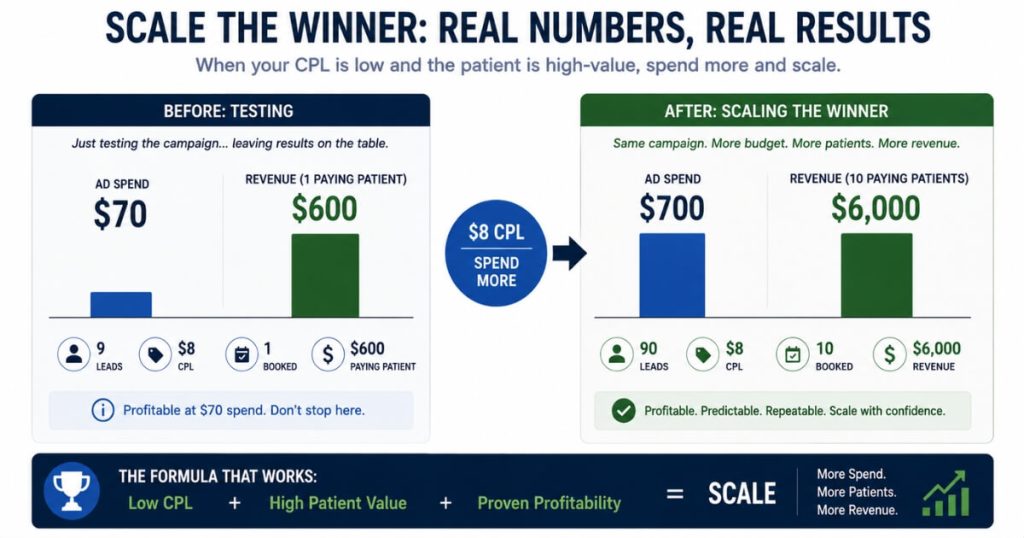
When should a clinic scale a campaign instead of pausing or fixing it?
Scale the moment a campaign produces cheap leads that book and pay.
Do not let a single conversion scare you into thinking it was a fluke.
The most common and expensive mistake we see is a clinic cutting the budget on a winner.
Picture a Facebook ad that produced:
- A paying patient at a $600 ticket
- About $70 of total spend
- An $8 cost-per-lead on the best ad
That is a five-to-six-times return.
The instinct of a nervous clinic is to slow down:
“It only worked once.”
Wrong direction.
When leads are cheap, people are booking, and people are paying, you spend more.
You do not optimize a winner.
You feed it.
Under-spending a profitable campaign is just as costly as over-spending a broken one.
Before you scale, isolate the winner.
Take the ad or ad set that produced the result.
Move it into its own campaign so its budget and data are not muddied by the underperformers around it.
Then put budget behind that clean campaign.
This is also why, when a clinic debates relaunching Google versus pouring more into a working channel, the answer is usually the working channel.
If TikTok is producing leads at four or five dollars and a paying patient is in sight, that beats rebuilding Google from zero.
Scaling a proven winner beats relaunching from scratch every time.
You already have evidence that the offer-creative-channel combination works.
We have watched this compound at scale.
A weight-loss and medspa clinic where we added $6.7M in revenue in one year across multi-channel paid ads grew by maximizing what worked before adding anything new.
Depth before width.
How can a clinic tell if low-quality leads are an ad problem or a sales problem?
Check the contact rate, not just the cost per lead.
Whether people answer the phone and text back tells you if the leads are real.
That separates an ad problem from a sales problem.
Cost per lead on its own is misleading.
A TikTok campaign can produce leads at four or five dollars each.
But if nobody has booked, the reflexive move is to blame the ad and start over.
Before you do, ask the diagnostic questions:
- Are people answering the phone?
- Are they texting back?
- Are they real human beings on the other end?
If patients are picking up and having real conversations but not converting yet, the leads are real.
The problem is downstream.
That usually means:
- Your sales cadence
- Your follow-up
- Your offer
Real people who answer but do not buy is a positive signal.
It means the top of your funnel works.
The fix lives in the conversion conversation, not the campaign.
If nobody ever answers and the numbers are fake or disconnected, then the targeting or platform is producing junk.
That is an ad problem you fix at the ad level with audience and creative changes.
There is also a quieter version:
An audience-language mismatch.
A South Florida clinic serving a heavily Spanish-speaking, expat-heavy market will see soft conversion if every intake form and follow-up message is English-only.
That is not the ad failing to find people.
It is the funnel failing to speak to them.
“Bad leads” is not a diagnosis.
It is a symptom.
The contact rate is the test that tells you which disease you actually have.
Should a clinic run leads to a landing page or an instant lead form on Google and TikTok?
Test both rather than presuming.
Instant forms usually produce cheaper, higher-volume leads.
A landing page usually produces fewer but higher-quality leads.
The right answer depends on what your sales operation can handle.
The textbook preference is a landing page.
With a landing page, you can:
- Control the page
- Track conversions cleanly
- Pre-qualify the buyer before they become a lead
But the field result is often different.
An instant lead form on TikTok or Facebook can deliver cheaper leads in higher volume.
If those leads are booking and paying, the landing page does not matter.
We tell clinics plainly:
If you are getting cheaper leads right now and they are booking and paying, keep doing what you are doing.
Do not “fix” a setup that is working just because a best-practices article told you to use a landing page.
The honest move is to split-test.
Clone the campaign.
Run:
- Half the budget to a landing page
- Half the budget to an instant form
Then let booking and payment data decide.
They are different campaigns with different objectives.
Judge them on cost per booked, paid patient.
Do not judge them only on cost per lead.
The deeper variable is your sales operation.
A clinic with a fast, disciplined follow-up team can win with cheap instant-form leads because it can work the volume.
A clinic with a thin sales operation is better off with fewer, more-qualified landing-page leads it can actually handle.
This is the same discipline that let an orthopedic surgical practice add $2M in revenue from Facebook ads alone— the offer, the funnel, and the follow-up dialed in together, not in isolation.
FAQ’s About Relaunching Underperforming Clinic Ads
How long should a cash-pay clinic give a new Google or TikTok campaign before judging it?
Give it enough spend to gather statistically meaningful data, not a fixed number of days.
That means budgeting a floor, not a ceiling.
The rule we use is this:
Do not spend less than about $20 a day on a new campaign.
Below that, the platform never gathers enough data to optimize.
At roughly a $20 cost-per-lead assumption, $20 a day is around $600 a month.
That is enough to collect real signal on whether the campaign produces leads.
The first thing a new campaign tells you is volume.
That answer usually arrives inside the first one to two weeks of consistent spend.
Bookings and paying patients take longer because they depend on:
- Follow-up
- Sales process
- Offer
The honest timeline is:
- 1 to 2 weeks to know if the campaign generates leads
- Another 2 to 4 weeks to know if those leads convert to paying patients
Do not judge a campaign on day three.
Do not cut budget on cheap leads just because no one has booked yet.
The booking problem usually lives downstream of the ad.
What signals tell a clinic to pause a campaign versus fix it versus fully relaunch it?
Pause when the platform itself is broken or spend is producing nothing.
Fix when leads are coming in but not converting.
Relaunch when the underlying offer, landing page, or campaign structure is wrong at the foundation.
A pause is a delivery problem.
Examples include:
- Budget cap
- Stalled delivery
- Account verification issue
- Leads dropping to zero overnight while spend continues
A fix is a conversion problem.
Leads arrive at a reasonable cost, but nobody books.
That points to follow-up, the sales script, or the offer.
A relaunch is a foundation problem.
If you need to swap the landing page, rebuild the form, and restructure the campaign, that is a relaunch.
The mistake is relaunching when you should fix, and pausing when you should scale.
What should a cash-pay clinic change first when ads underperform — offer, creative, landing page, or audience?
Fix the plumbing and follow-up first.
Before changing the offer, creative, or audience, confirm:
- The booking calendar works
- Lead notifications reach your sales rep
- The CRM is capturing leads
- Automations are not breaking the funnel
Then fix follow-up speed and the sales process.
Only after that should you change the funnel itself.
Use this order:
- Landing page versus instant form
- Offer
- Creative
- Audience
Change one variable at a time so you know what moved the number.
When should a clinic scale a campaign instead of pausing or fixing it?
Scale the moment a campaign produces cheap leads that book and pay.
Do not assume one conversion was a fluke.
If an ad produces:
- A paying patient
- Cheap leads
- A profitable return
you spend more.
Before scaling, isolate the winner.
Move the winning ad or ad set into its own campaign.
Then put budget behind that clean campaign.
Scaling a winner beats relaunching from scratch because you already have proof the combination works.
Depth before width.
How can a clinic tell if low-quality leads are an ad problem or a sales problem?
Check the contact rate.
If people answer the phone and text back, the leads are real.
If they are not converting, the issue is downstream:
- Sales process
- Follow-up cadence
- Offer
If nobody answers and the numbers are fake or disconnected, it is probably an ad problem.
That means targeting or platform quality needs to be fixed.
Cost per lead alone does not tell the full story.
Contact rate does.
Should a clinic run leads to a landing page or an instant lead form on Google and TikTok?
Test both.
Instant forms usually produce cheaper, higher-volume leads.
Landing pages usually produce fewer but higher-quality leads.
The right answer depends on your sales operation.
A clinic with fast, disciplined follow-up can win with cheap instant-form leads.
A clinic with a thin sales team may need fewer, more-qualified landing-page leads.
Clone the campaign.
Run half the budget to each.
Then judge by cost per booked, paid patient — not cost per lead.