What Does a Cash-Pay Clinic Need in Place Before Running Facebook Ads?
Roughly nine out of ten cash-pay medical practices that come to us asking about Facebook ads are not actually ready to run them.
The ones that launch anyway burn cash, blame the platform, and conclude that “ads don’t work for clinics.”
The truth is that Meta ads are a multiplier, not a starting engine. They amplify whatever you already have.
If your offer is profitable, your follow-up is fast, and your brand holds up to a quick Google search, ads pour fuel on it.
If any of those are missing, ads just expose the leak faster.
This is the concrete checklist — offer, landing page, closer, speed-to-lead, tracking, and compliant creative — of what a cash-pay clinic needs in place before spending a single dollar on Facebook or Instagram.
How much should a clinic budget for Facebook ads before it’s ready?
Plan for at least $3,000–$5,000 a month in ad spend for a meaningful test.
Do not turn on ads until your offer can pay that back.
Meta needs roughly 50 conversions per ad set per week to exit its learning phase and optimize properly.
A budget too small to generate that data never gets out of learning. It produces expensive, random results.
So underfunding a test is not “being careful.”
It is guaranteeing a bad answer.
The number that decides readiness is not the budget, though.
It is whether a single converted patient covers:
- Your ad spend
- Your agency or management cost
- Your required profit
That is why the offer comes first.
If the offer you are advertising carries at least $5,000 in lifetime value, one closed patient can cover the cost of acquiring several leads and still leave profit.
That means the patient spends at least five grand with you across the time they stay a customer.
If your offer cannot clear that bar, you are trapped in a low-margin loop.
Every patient barely pays for the next.
No amount of budget tuning fixes that.
Fix the offer’s economics before you fix the campaign.
For the full picture of how cash-pay clinics structure offers and channels, our med spa marketing hub lays out the system end to end.
Do I need a landing page or can I just run Facebook ads to my website?
You need a dedicated landing page or funnel.
Sending paid traffic to your homepage is one of the fastest ways to waste ad spend.
A homepage is built for browsing.
It gives a visitor a dozen places to click and no single decision to make.
As a result, paid traffic scatters and cost-per-lead climbs.
A landing page does the opposite.
It gives the visitor:
- One offer in the headline
- Proof directly beneath it
- One action to take
That action may be:
- A form
- A quiz
- A scheduler
The page should restate the exact offer from the ad.
That way, the message matches what made the person tap.
It should also load fast on mobile, because that is where the traffic is.
Finally, it should drop every lead straight into your CRM.
Match the funnel to your bottleneck
There is no universally “best” funnel.
There is only the funnel that fits what you need right now.
- Native lead form: keeps cost-per-lead low and volume high
- Landing page: raises lead quality because the visitor has to engage with the offer
- Scheduling page with a credit-card hold: filters down to people genuinely ready to book and weeds out tire-kickers
Choose based on whether your bottleneck this month is volume or quality.

Why do I need a dedicated closer before running ads?
Because paid leads convert on the strength of the follow-up.
A receptionist juggling the front desk cannot do that job.
You need one person whose actual role is closing.
Not:
- A receptionist
- A part-timer
- Someone splitting attention across phones and check-ins
Make them commission-based so they have skin in the game.
Train them on:
- Objection handling
- Urgency
- Relationship building
- Hospitality
- Empathy
Give them:
- A proven script
- A CRM workflow
- A clear conversion target
That way, you can hold them accountable to conversion rate, not just show rate.
That distinction matters.
Show rate tells you people arrived.
Conversion rate tells you they bought.
Paid leads are colder and more skeptical than the word-of-mouth referrals most clinics are used to closing.
The person did not come from a friend’s recommendation.
They came from an ad, on impulse, and they are comparing you to three other clinics.
That makes the close harder.
It also makes first contact more important.
Without a dedicated closer, you spend money generating leads you fail to turn into revenue.
It reads like an ad problem.
Really, it is a sales-infrastructure problem.
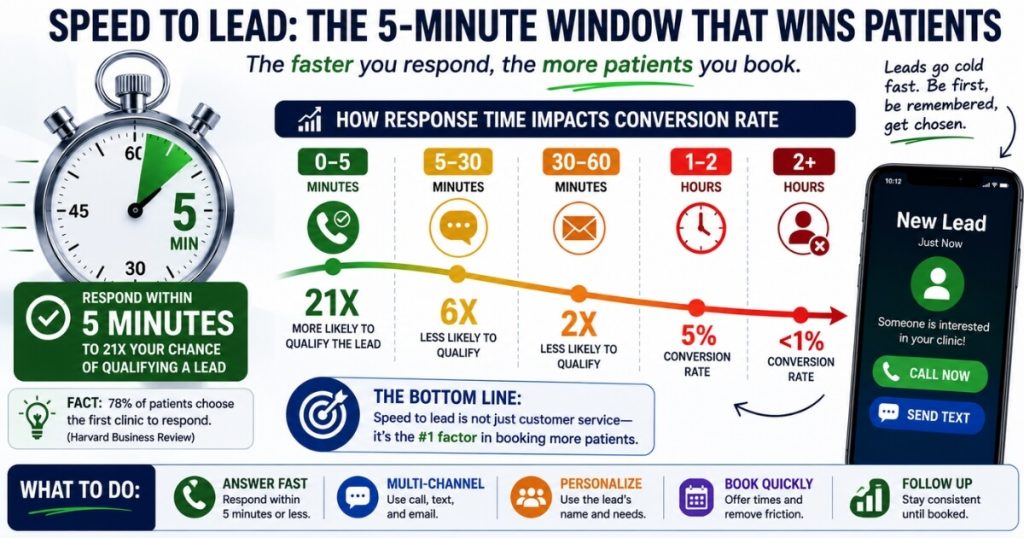
How fast do I have to follow up with Facebook leads?
Within five minutes, and ideally immediately.
Speed-to-lead is the single biggest lever on the conversion of paid traffic.
A Meta lead saw your ad, tapped a button, and was back to scrolling within seconds.
The intent is real, but it decays by the minute.
Clinics that call back in minutes book dramatically more of the exact same leads than clinics that respond in hours.
By the next day, the prospect may have:
- Forgotten the ad
- Submitted three competitors’ forms
- Lost the impulse that made them act
So the infrastructure has to fire instantly.
You need:
- Lead notifications that hit your closer’s phone the second a form is submitted
- An automated text or email that goes out immediately
- A closer who can pick up the phone fast
This is non-negotiable for high-ticket cash offers.
Cash needs to come in as fast as you are putting it out.
Slow follow-up is exactly where that money quietly leaks.
What tracking do I need set up before launching Meta ads?
At minimum, you need:
- The Meta Pixel
- The Conversions API
- A CRM capturing every lead
- A way to attribute booked and paid patients back to the ad
Without tracking, you are flying blind.
You will see clicks and form-fills in Meta’s dashboard.
But you will not know which campaign produced an actual paying patient.
And the paying patient is the only number that matters when you are spending real money.
Vanity metrics like cost-per-lead can look great while the campaign quietly loses money on patients that never close.
Because Meta has lost a lot of browser-based signal to privacy changes, server-side Conversions API is no longer optional.
Connect the pixel and CAPI to your CRM so down-funnel events feed back to Meta.
Those events include:
- Booked consult
- Showed
- Paid
Once the algorithm can see who actually buys, it stops optimizing toward cheap leads.
It starts finding people who convert.
That feedback loop is what separated the multi-channel paid program at NuLevel Wellness Medspa, where dialed-in tracking and follow-up helped drive $6.7M a year and 3,727 new patients, from clinics that spend the same money and never know what worked.
Why does my brand and online reputation matter before I run ads?
Because almost every ad-driven lead Googles your clinic before they book.
A sketchy online presence kills the conversion no matter how good the ad is.
Even if you run a killer offer ad and it goes viral, the journey does not end at the click.
The interested person opens a new tab and searches your name.
If they find:
- Outdated information
- No reviews
- A dated site
- An untrustworthy online presence
they bounce.
You paid for that click.
The ad gets the click.
The brand gets the booking.
So before you spend, build the conversion infrastructure:
- A professional, modern website
- A verified and optimized Google Business Profile
- Real five-star reviews from real patients
- An SEO presence so you also show up organically
- A working CRM behind all of it
This is also why creative has to be compliant.
Meta is strict on healthcare and personal-health claims.
So lead with:
- Patient stories
- Clear offers
- Provider credibility
Avoid:
- Before-and-afters
- “Cure” language
- Claims that get accounts flagged
You cannot out-spend a weak brand or a banned ad account.
When the offer, follow-up, and brand are all in place, dialed-in Facebook is what produced an orthopedic surgical center that added $2M in revenue from Facebook ads alone.
FAQ’s About Getting Ready to Run Facebook Ads
How much should a clinic budget for Facebook ads before it’s ready?
Plan for at least $3,000–$5,000 a month in ad spend for a meaningful test.
Do not turn on ads until your offer can pay that back.
Meta needs roughly 50 conversions per ad set per week to optimize.
A budget too small to generate that data will never exit the learning phase.
It will produce expensive, random results.
The deeper readiness question is not the size of the budget.
It is whether one converted patient covers:
- The spend
- The agency or management cost
- A profit margin
If your offer carries at least $5,000 in lifetime value, a single closed patient can carry the cost of acquiring several leads.
That is what makes the math survive.
If your offer cannot do that, no budget is the right budget.
You are funding a low-margin loop where every patient barely pays for the next one.
Do I need a landing page or can I just run Facebook ads to my website?
You need a dedicated landing page or funnel.
Sending paid traffic to your homepage is one of the fastest ways to waste ad spend.
A homepage is built for browsing and offers a dozen exits.
A landing page is built for one decision and one action.
It should include:
- The offer in the headline
- Proof beneath it
- A single form or scheduler
The page must load fast on mobile.
It must restate the exact offer from the ad.
It must pass the lead straight into your CRM.
Lead forms keep cost-per-lead low and volume high.
Landing pages raise quality.
Scheduling pages with credit-card holds filter down to people genuinely ready to book.
Choose based on whether you need volume or quality right now.
Why do I need a dedicated closer before running ads?
Because paid leads convert on the strength of the follow-up.
A receptionist juggling the front desk cannot do that job.
You need one person whose actual role is closing.
Ideally, they should be commission-based so they have skin in the game.
They should be trained on:
- Objection handling
- Urgency
- Relationship building
- Hospitality
- Empathy
They should work from:
- A proven script
- A CRM workflow
That structure lets you hold them accountable to conversion rate, not just show rate.
Paid leads are colder and more skeptical than referrals.
So the close is harder, and the speed of first contact matters more.
Without a dedicated closer, you generate leads you cannot turn into revenue.
That looks like an ad problem, but it is actually a sales-infrastructure problem.
How fast do I have to follow up with Facebook leads?
Within five minutes, and ideally immediately.
Speed-to-lead is the single biggest lever on paid traffic conversion.
A Meta lead saw your ad, tapped a button, and moved on within seconds.
The intent is real, but it decays by the minute.
Clinics that call back in minutes book dramatically more of the same leads than clinics that respond in hours.
Set up:
- Instant lead notifications
- Automated text or email
- A closer who can call back fast
For high-ticket cash offers, cash needs to come in as fast as you are putting it out.
Slow follow-up is where most of that money quietly leaks.
What tracking do I need set up before launching Meta ads?
At minimum, install and configure:
- Meta Pixel
- Conversions API
- CRM lead capture
- Attribution from ad to booked and paid patients
Without this, you are flying blind.
You will see clicks and form-fills, but not which campaign produced an actual paying patient.
Because Meta has lost a lot of browser-based signal to privacy changes, Conversions API server-side tracking is no longer optional.
Connect the pixel and CAPI to your CRM.
Then send down-funnel events like:
- Booked consult
- Paid
back to Meta.
That helps campaigns optimize toward buyers instead of form-fills.
Why does my brand and online reputation matter before I run ads?
Because almost every ad-driven lead Googles your clinic before they book.
If your online presence looks weak, they bounce.
You need:
- A professional, modern website
- A verified and optimized Google Business Profile
- Real five-star reviews
- An SEO presence
- A working CRM
Think of this as your conversion infrastructure.
The ad gets the click.
The brand gets the booking.
You cannot fix a weak brand by spending more on ads.