How Can a CRM Lower Patient Acquisition Cost for a Cash-Pay Clinic?
Most cash-pay clinics try to lower their patient acquisition cost by chasing cheaper ads.
The faster path is almost always the opposite end of the funnel — the leads you already paid for and never converted.
A CRM does not make a single click cheaper. It lowers your CAC by converting more of the same traffic: catching every lead the moment it arrives, following up before it goes cold, plugging the leaks where paid leads quietly disappear, and reactivating a database you have been sitting on.
This is the concrete answer to how a CRM cuts patient acquisition cost at a cash-pay clinic, and why it is usually the highest-return change you can make before you touch your ad budget.
What actually drives patient acquisition cost — and why a CRM moves it
Patient acquisition cost is total spend divided by patients booked, and a CRM lowers it by raising the second number, not lowering the first.
This is the part most clinics miss.
They treat CAC as a media problem. They look for cheaper leads and hunt for a lower cost per click.
In reality, the bigger lever sits in conversion.
If you spend the same money but book more of the leads it generates, your CAC falls just as surely as if your ads got cheaper. Usually, it falls faster.
Here is the math that makes it real:
- Spend: $10,000
- Leads generated: 100
- Booked patients: 8
- CAC: $1,250
Now keep everything the same:
- Spend: $10,000
- Leads generated: 100
- Booked patients: 14
- CAC: roughly $714
That is a CAC reduction of more than 40%.
Nothing about the traffic changed.
What changed is how much of it survived the gap between “submitted a form” and “showed up and paid.”
A CRM is the system that closes that gap on purpose instead of leaving it to a busy front desk.

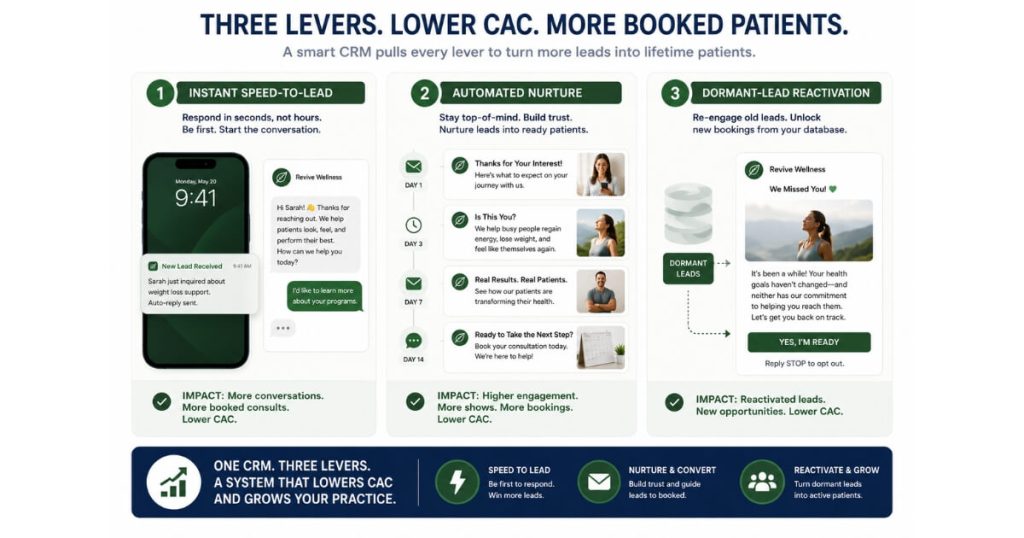
Speed-to-lead — the cheapest CAC win there is
The single fastest way a CRM lowers CAC is by responding to every lead in minutes instead of hours, because a cash-pay lead is hottest the instant they hit submit.
Contact rates collapse with delay.
A lead answered in the first few minutes is dramatically more likely to connect and book than the same lead called back the next morning.
A clinic relying on manual follow-up almost never hits that window because the front desk is:
- On the phone
- Checking patients in
- Running the floor
A CRM removes the human bottleneck from first contact.
The moment a lead arrives — from a Facebook form, a Google landing page, a TikTok offer, or anywhere else — it can:
- Fire an instant text
- Send an email
- Alert the team
- Drop the patient onto a booking calendar
All before anyone lifts a finger.
That recovered contact rate is pure CAC reduction.
You are converting leads you already paid for that would otherwise have gone cold by default.
It is one of the few levers that costs nothing extra in ad spend and pays back immediately.
Nurture — converting the “not yet” leads instead of rebuying them
Most leads do not book on the first touch, and a CRM lowers CAC by nurturing them to a decision automatically rather than letting you pay for the same lead twice.
Cash-pay treatments often involve weeks of consideration.
This is especially true for:
- TRT
- Hormone programs
- Regenerative pain
- Functional medicine
- Higher-ticket aesthetics
The patient is interested but not ready.
Without follow-up, they simply evaporate.
Then the clinic spends fresh ad dollars to acquire a brand-new lead in exactly the same headspace.
A CRM runs the long game on autopilot.
Multi-step text and email sequences keep the clinic in front of the lead with:
- Education
- Social proof
- Offers
These sequences can continue for days or weeks until the patient books or opts out.
None of that follow-up consumes new ad spend.
As a result, every patient nurtured into a booking lowers your blended acquisition cost.
This is the difference between a clinic that “needs more leads” and one that quietly converts the leads it already has.
The no-leak pipeline — stop paying for leads that fall through the cracks
A leaky pipeline inflates CAC invisibly, and a CRM lowers it by making sure no paid lead exits the process without a decision.
Every clinic has leaks.
Examples include:
- Form fills no one called
- Consults that never got a follow-up
- No-shows no one rebooked
- Quotes that were never chased
Each one is money spent on a lead that produced nothing.
Because the spend is already sunk, the loss rarely shows up as an obvious line item.
Instead, it appears as a higher CAC that nobody can explain.
A CRM turns the pipeline into tracked stages.
Each stage has:
- An owner
- An automated next action
No lead sits without a follow-up task.
No-shows trigger an automatic rebooking sequence.
Stalled deals resurface instead of disappearing.
When the leaks close, the same volume of paid leads produces more booked patients.
CAC drops without buying a single additional click.
A no-leak pipeline is the structural backbone of cost-efficient patient acquisition for cash-pay clinics.
It is exactly the kind of system we build before we ever recommend spending more.
Reactivation — mining the leads you already paid for
The cheapest acquisition source a clinic owns is its own database, and a CRM lowers CAC by turning dormant leads, no-shows, and lapsed patients back into bookings at near-zero marginal cost.
Every old lead already cost money to acquire once.
A reactivation campaign can be as simple as:
- A text message
- An email
- A new offer
sent to dormant leads.
Because there is no new ad spend behind it, the bookings cost a fraction of what a new lead costs.
The revenue is recovered, not rebought.
This is often the highest-return move a clinic has never made.
Why?
Because the leads live in:
- Spreadsheets
- Inboxes
- The front desk’s memory
instead of a system that can message the entire database with one campaign.
A CRM holds the asset and lets you mine it on demand.
Treat the database as something you reactivate repeatedly rather than a funnel you run once.
When you do, recovered revenue becomes one of the largest and most reliable CAC reductions available.
Source attribution — cut the channels that are quietly bleeding you
A CRM lowers CAC by tracking every lead from its source all the way to booked revenue, so you can finally see true cost per acquisition by channel instead of optimizing to the cheapest lead.
Cheapest lead is a trap.
A channel that produces $20 leads that never book has a worse CAC than a channel with $80 leads that convert three times better.
Without closed-loop tracking, clinics keep pouring budget into the cheap-lead channel because the per-lead number looks good.
Meanwhile, their blended CAC stays stubbornly high.
A CRM fixes that.
By tagging every lead with its source and following it all the way to revenue, a CRM shows which channels actually produce paying patients.
Then the decision becomes obvious:
- Reduce spend on high-CAC channels
- Increase spend on proven channels
That reallocation lowers your blended acquisition cost without increasing budget.
It simply spends the existing dollars where they convert.
What this looks like when it is working
The clinics that get this right do not grow by outspending competitors — they grow by converting far more of the same spend, and the results compound.
When the CRM is:
- Catching every lead in minutes
- Nurturing the not-yet buyers
- Plugging pipeline leaks
- Reactivating the database
every channel above it performs better because nothing downstream is wasted.
At Eternity Health Partners, that combination helped take the practice from $1M to $4M while consistently fielding around:
- 60 inbound calls per month
- 40 web leads per month
Leads that a no-leak system actually converts instead of dropping.
At VYVE Wellness, a 900% increase in leads and 100-plus inbound calls per month only translated into growth because the intake and follow-up system could absorb the volume without leaking.
More leads with a broken pipeline raises CAC.
More leads with a CRM behind them is how you lower it.
FAQ’s About CRMs and Patient Acquisition Cost
Does a CRM lower patient acquisition cost or just organize my leads?
It does both.
The organizing is what lowers the cost.
Cost per acquisition equals total spend divided by patients booked.
A CRM does not make your ads cheaper.
Instead, it converts more of the leads you already paid for.
When speed-to-lead, nurture, and a no-leak pipeline turn 8 booked patients out of 100 leads into 14 from the same 100 leads, CAC drops by roughly 40%.
A CRM is not just a contact list with reminders.
It is the conversion layer that determines how much of your ad budget becomes revenue.
How fast does speed-to-lead have to be to matter for a cash-pay clinic?
Minutes, not hours.
A cash-pay lead is hottest the moment they submit the form.
Contact rates fall sharply with every minute of delay.
A CRM closes that gap automatically by:
- Sending a text
- Sending an email
- Alerting the front desk
- Routing the lead to a calendar
Manual follow-up cannot compete.
A front desk juggling phones and check-ins often reaches the lead hours later.
By then, the patient has booked elsewhere or gone cold.
What is a leaky pipeline and how does a CRM stop the leaks?
A leaky pipeline is every place a paid lead falls out of the process without a decision.
Examples include:
- Form fills no one called
- No-shows no one rebooked
- Consults without follow-up
- Quotes that were never chased
A CRM stops those leaks by giving every lead:
- A tracked stage
- An owner
- An automated next action
When the pipeline stops leaking, the same ad spend produces more booked patients and CAC falls.
Can a CRM bring back leads I already paid for but never converted?
Yes.
In fact, that database is usually the cheapest acquisition source a clinic has.
Every old lead, no-show, and lapsed patient already cost money to acquire.
A CRM lets you reactivate them with automated nurture and offer campaigns at virtually zero marginal cost.
The clinics that win on CAC treat their database as an asset they mine repeatedly, not a one-time funnel.
How does a CRM tell me which marketing channels to cut?
By tracking every lead from source to booked revenue.
Most clinics optimize for cost per lead.
That is a mistake.
A channel with cheap leads that never book can have a terrible CAC.
A channel with more expensive leads that convert can be your most profitable source.
A CRM closes the loop between spend and revenue.
It shows which channels actually produce paying patients.
Then you can move budget into what works and away from what does not.
That lowers blended acquisition cost without spending an extra dollar.
The next step
If your patient acquisition cost feels too high, the answer is probably not cheaper ads.
It is converting more of the leads you are already paying for.
Speed-to-lead, automated nurture, a no-leak pipeline, database reactivation, and true source attribution are the levers.
A CRM is the system that pulls all five at once.
Most clinics are leaving the largest CAC reduction of their year sitting in a spreadsheet full of leads they never followed up with.
If you want someone to look at your funnel, your follow-up, and your channel mix together — and show you exactly where your acquisition cost is leaking — that is the conversation to book.
We will map where your spend is being lost and what a CRM-backed pipeline would recover.