What Profit Margin Should You Expect on a GLP-1 / Semaglutide Program?
Almost every cash-pay clinic asks the wrong version of this question. They want to know the gross margin on the semaglutide itself — cost of goods versus the monthly price — and then they build their entire business on that one thin number.
The front-end GLP-1 margin is fine. It is not the answer.
After dozens of discovery calls with clinics across the country, the pattern is brutally consistent: practices collect roughly $600 in profit over the first three or four months, lose the patient around day 90, and then spend money to buy a replacement.
This is the FAQ on what margin to actually expect on a GLP-1 program — the front-end numbers, how to price it, and where the real profit lives.
What gross profit margin should a cash-pay clinic expect on a GLP-1 / semaglutide program?
On the front-end GLP-1 script alone, expect to price the program at roughly $400 to $600 per month and keep $600 to $1,500 in profit across the first four months.
On the typical $1,600 to $2,400 collected over those four months, that puts the gross margin somewhere in the 35% to 65% range depending on your vendor and your cost of goods.
That is a perfectly healthy product margin.
The problem is not the margin itself — it is treating that first-quarter profit as the whole prize.
The most common economic model we see on discovery calls is:
- Collect the GLP-1 money for three or four months
- Lose the patient
- Spend again to acquire a new one
That margin is real, but it is shallow, and it caps your practice at the cost of constantly re-buying patients.
The clinics that win do not get a better price on semaglutide — they get more months of care out of every patient they already paid to acquire.
How should you price a GLP-1 program — membership vs one-off?
Price it as a membership, not a one-off script refill.
The membership model of cash flow is what converts a GLP-1 program from a commodity into a high-LTV recurring business.

A clean structure looks like this:
- Months 1-4: $400 to $600 per month on the GLP-1 itself
- Months 5-8: $300 to $700 per month for the next phase of care
- Months 9-12: $300 to $700 per month for the back half of the year
The reason membership beats one-off pricing has nothing to do with the price tag and everything to do with expectations.
When a patient signs up for a program rather than a prescription, you have earned permission — from day one — to:
- Run labs again
- Hold another consultation
- Present the next phase of care
And none of it lands as a hard upsell.
One-off pricing does the opposite. It trains the patient to leave the moment the weight comes off, which is exactly the fall-off pattern crushing most clinics today.
If you want the broader playbook on building these offers, our med spa marketing approach is built around recurring membership economics rather than one-and-done treatments.
Where is the real profit in a GLP-1 / semaglutide program?
The real profit is downstream lifetime value — retaining, upselling, and cross-selling the patient you have already paid to acquire.
The name of the game in cash-pay medicine is patient acquisition. Once you have acquired a GLP-1 patient, the expensive part is done. Every additional month of care is profit you do not have to spend ad dollars to earn.
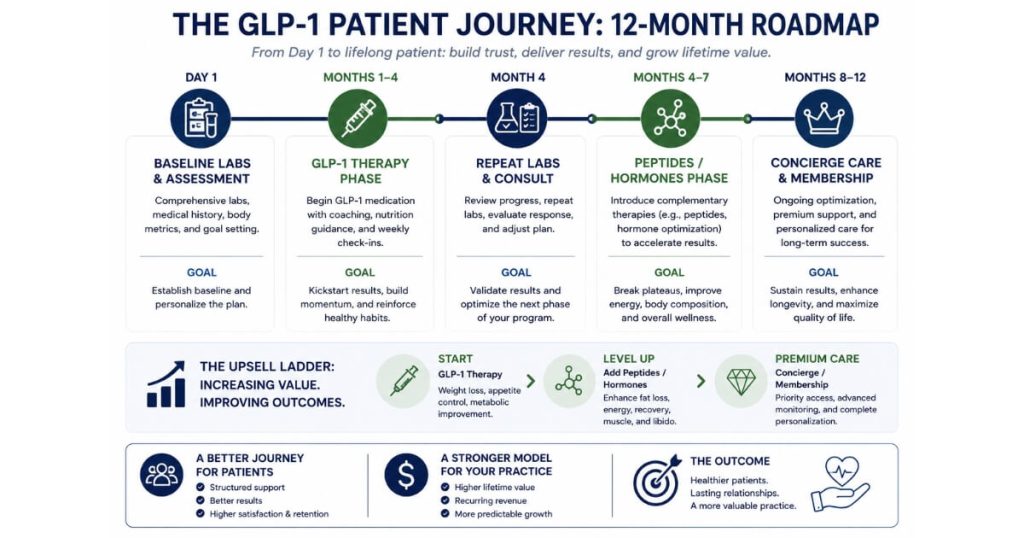
Here is the journey that unlocks it:
- The patient completes the first four months on the GLP-1.
- The patient moves into the next phase of care.
- That phase may include:
- Peptides
- Hormones
- A concierge program if you do not stock all of those medications
- The patient pays $300 to $700 per month.
- You typically keep $800 to $2,000 over that four-month block.
- You repeat the cycle for months eight through twelve.
You do not have to invent demand for any of this.
You have already built the relationship. The patient is already healthier and bought-in.
The contrast is stark:
- A clinic that only collects the GLP-1 money keeps about $600 in year one and then has to buy a new patient.
- A clinic that runs the full journey keeps roughly $2,200 in year one from the same patient.
Many of those patients stay for years.
This is the same compounding we saw at a weight-loss and medspa clinic where we added $6.7M in revenue in one year across 3,727 new patients. The front-end weight-loss offer was the entry point, but the revenue compounded because the patients did not fall off after the first quarter.
The profit is not in the drug.
It is in the relationship the drug lets you open.
How do labs improve the margin on a GLP-1 program?
Labs are the cheapest selling opportunity you can buy.
A baseline panel runs roughly $150 to $200, and rather than billing it separately you simply build that cost into the program price.
Labs at intake confirm the patient is actually a fit.
Repeating labs at the end of month four creates a natural, non-salesy reason to have another consultation — ideally a real 60-minute conversation if you want to build high lifetime value.
The blood work does the selling for you.
Instead of you trying to convince the patient to keep spending, the labs report what is happening inside their body. You then co-diagnose and present treatment options.
That reframes the entire decision.
The patient is now choosing between you and you, rather than choosing between you and your competitor down the street.
Even if repeat labs only convert one in four GLP-1 patients into the next phase of care, the math still moves hard in your favor.
The cost of creating that opportunity is a couple hundred dollars — not a fresh patient-acquisition spend.
Why do most clinics lose money on GLP-1 patients after 90 to 120 days?
Because they do nothing with the patient after the first three or four months.
The industry-wide trend right now is patients falling off after the first one to four months of a weight-loss program.
Most clinics simply take the roughly $600 in first-quarter profit and walk away.
That leaves the practice on a treadmill:
- Collect a thin margin
- Lose the patient around day 90 to 120
- Spend on ads to acquire a replacement
It is an exhausting, capped way to run a business.
The fix is operational, not clinical.
- Set the expectation of ongoing care at the first consultation.
- Schedule repeat labs at month four before the patient has any reason to drift.
- Build a real service ladder behind the first visit.
That ladder may include:
- Peptides
- Hormones
- Concierge care
Clinics without that ladder are effectively renting patients.
Clinics with it own them.
What is a realistic first-year profit per GLP-1 patient when you run the full journey?
Running the full journey, a realistic and deliberately conservative first-year retained profit is around $2,200 per patient — versus about $600 for a clinic that only sells the GLP-1 and then loses the patient.
The conservative build is straightforward:
- Keep $800 across the GLP-1 and first upsell phase.
- Keep another $800 across the back half of the year on the higher-margin care.
- Keep roughly $600 on the remaining blocks.
That lands near $2,200.
Critically, you spend nothing to re-acquire that patient to earn it.
Because many of these patients stay for multiple years, the multi-year LTV is a multiple of the first-year figure.
The same compounding logic shows up across the cash-pay space.
At VYVE Wellness, a longevity and functional-medicine clinic, we drove a 900% lead increase and over 100 inbound calls a month precisely because the offer was built to retain and ascend patients, not to sell a single transaction.
The headline number is not the GLP-1 margin.
It is that the same acquired patient is worth roughly three to four times more when you run the journey than when you sell the script and stop.
FAQ’s About GLP-1 Program Profit Margins
Is a 35%–65% gross margin on semaglutide good?
It is a healthy product margin.
However, it is the wrong number to optimize.
The front-end GLP-1 margin will never be your competitive advantage because every clinic buys from similar vendors.
Your advantage is:
- Retention
- Ascension
- Higher-margin care after the GLP-1
Optimize lifetime value, not the per-vial spread.
Should I charge separately for labs?
No.
Build the roughly $150 to $200 lab cost into the program price.
Billing labs separately creates friction and discourages the repeat testing that drives your next selling opportunity.
Bake it in so labs feel like part of the care, not an add-on fee.
What do I upsell GLP-1 patients into?
Typical next steps include:
- Peptides
- Hormones
- A concierge program
If you do not stock those medications, move the patient onto a concierge model and transfer their standard care to you, including nurse-practitioner and PA visits.
The goal is simple:
- Retain the patient
- Upsell the patient
- Cross-sell the patient
Do not let them fall off and force you to buy a replacement.
How long do GLP-1 patients stay if I run the journey?
The conservative model assumes a full first year.
Many patients stay for years once you:
- Set the expectation of ongoing care
- Run labs regularly
- Give them a service ladder to ascend
Multi-year retention is what makes the LTV math compound far beyond the $2,200 first-year figure.
Why is patient acquisition the whole game?
Because acquiring a new cash-pay patient is the single most expensive thing your clinic does.
Once you have paid to acquire a GLP-1 patient, every additional month of care you sell is profit you did not have to spend ad budget to earn.
That is why the clinics that retain and ascend win.
They spread acquisition cost across years of care instead of a single quarter.
What’s the next step?
If your GLP-1 program is running on the front-end margin alone — collecting $600 over the first quarter and losing the patient by day 90 — you are leaving the majority of the profit on the table.
The fix is not a better price on semaglutide.
It is a membership structure, a labs cadence that creates selling opportunities, and a service ladder that turns a weight-loss patient into a multi-year, high-LTV relationship.
That is the difference between keeping $600 and keeping $2,200 in year one from the exact same patient.
If you want someone to look at your GLP-1 pricing, your upsell ladder, and your retention numbers together — and tell you exactly where the leverage is — that is the conversation to book.
We will map the full patient journey and the real LTV math for your practice on the call.