What ROAS Should a Cash-Pay Medical Practice Expect From Paid Ads?
Every cash-pay clinic owner wants one number: the ROAS — return on ad spend — they should expect from paid ads. The honest answer is that there is no single universal multiple. The realistic target is set by your ticket size, your margin, and your payback window, not by a benchmark borrowed from a different business. But there are real ranges, real payback timelines, and a short list of inputs that decide whether your account prints money or burns it. In one year we added $5 million in aggregate revenue across three cash-pay clinics by fixing those inputs. This is the concrete answer on what ROAS to expect by treatment and ticket, how fast it should pay back, and what separates a profitable ad account from a money pit.
What ROAS should a cash-pay medical practice realistically expect from paid ads?
A healthy cash-pay clinic should expect a blended 3x to 5x ROAS on front-end revenue from a dialed-in paid ad account. The number is substantially higher when you measure the full lifetime value of the patient instead of the first transaction.
The first-purchase ROAS is the number most clinics fixate on. However, it is the wrong one to optimize against for cash-pay care.
Most of these treatments recur or upsell. As a result, a 2x first-purchase ROAS can become a 6x to 10x ROAS once the second visit, the program, and the retention revenue are counted.
The right way to read the number depends on the offer.
A low-ticket aesthetic offer like a $300 filler special might run at break-even or a 1x to 2x ROAS on the front end. The entire point of the offer is to acquire the patient cheaply and earn on the back end.
A high-ticket program like a $15K-$25K neuropathy or joint-pain plan can show a 4x to 8x ROAS on the very first sale. The ticket is large enough to absorb the ad cost and still print a margin.
There is no single universal ROAS. The realistic target is set by your ticket, your margin, and your payback window, not by a generic benchmark.
We added $5 million in aggregate revenue across three cash-pay clinics in a single year by fixing the inputs that drive ROAS, not by chasing a magic number.
If you are building a full channel strategy around these economics, start with the medical practice marketing fundamentals. Then set a ROAS target per offer.
How does expected ROAS change by treatment and ticket size at a cash-pay clinic?
ROAS scales with ticket size and margin. That means the realistic target is different for a $300 filler offer than for a $20K pain program. Reading them with the same benchmark is how clinics misjudge a profitable account.
Low-ticket aesthetic and weight-loss front-end offers — filler, lasers, a GLP-1 starter month — are designed to acquire cheaply. As a result, a 1x to 2x first-purchase ROAS is normal. The profit lives in the recurring and upsell revenue behind the first visit.
Mid-ticket cash offers in the $3K to $20K range — body contouring, joint pain, neuropathy, and regenerative programs — should clear a 3x to 6x ROAS on the front end. The ticket is large enough to carry the ad cost while still leaving margin.
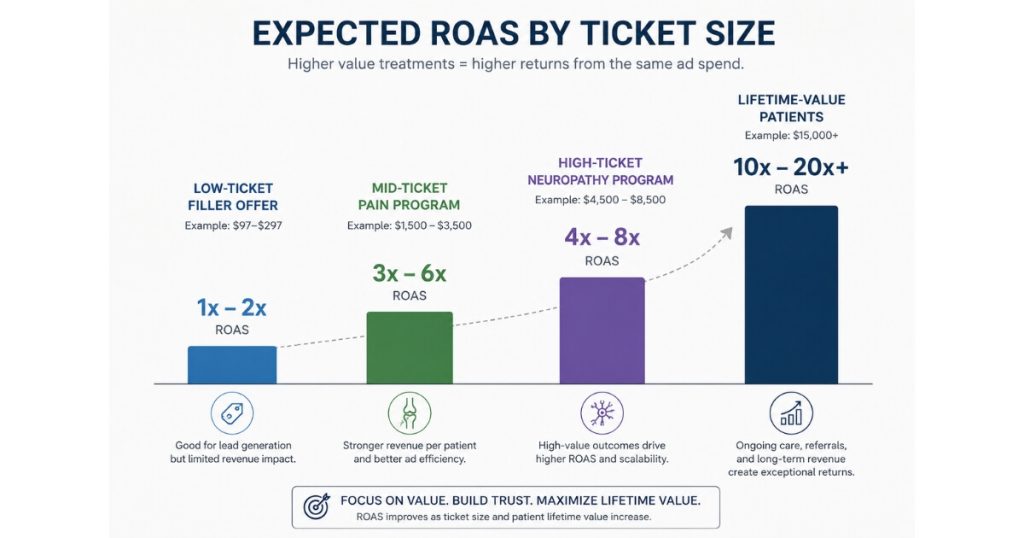
High-ticket programs above $20K, like long-form neuropathy and knee-pain plans, can show a 4x to 8x first-sale ROAS. However, they require fast follow-up and a real sales process to hit it.
Recurring high-LTV care like TRT and HRT often looks modest on first-purchase ROAS. However, it looks exceptional on lifetime ROAS because the patient pays monthly for years.
Pick the ROAS target that matches the ticket and the payback window for that specific offer. Do not use a blended number borrowed from a different vertical.
How long is the payback period on paid ads for a cash-pay medical practice?
For most cash-pay offers, the payback window should be measured in days to a few weeks, not months.
If your ad account cannot recover its spend that fast, the problem is usually the offer, the follow-up, or the cash conversion. It is rarely the ad platform.
The rule for high-ticket front-end cash offers like joint pain and neuropathy is blunt. Cash needs to come in roughly as fast as you are putting it out.
That is why these accounts cannot run without a fast follow-up operation. The lead needs to convert into a paid appointment within days.
Aesthetic and weight-loss offers can carry a slightly longer payback period. The front end is intentionally cheap, and the real return arrives on the second visit and the program upsell.
Recurring care like TRT, HRT, and concierge pays back the acquisition cost quickly. The appointments are paid, and the patient stays for months or years.
As a result, you recover spend in the first cycle or two and profit on everything after.
The clinics that get the payback timing wrong are almost always the ones with no nurturing and no front-desk follow-up SOPs. The leads come in. Nobody works them fast enough. The cash that should have closed the gap never shows up.
What separates a profitable cash-pay ad account from a money pit?
Four things separate a profitable account from a money pit:
- The offer matches the most profitable patient type.
- The targeting is precise.
- There is real mid-funnel nurturing.
- The front desk has follow-up SOPs that turn appointments into cash.
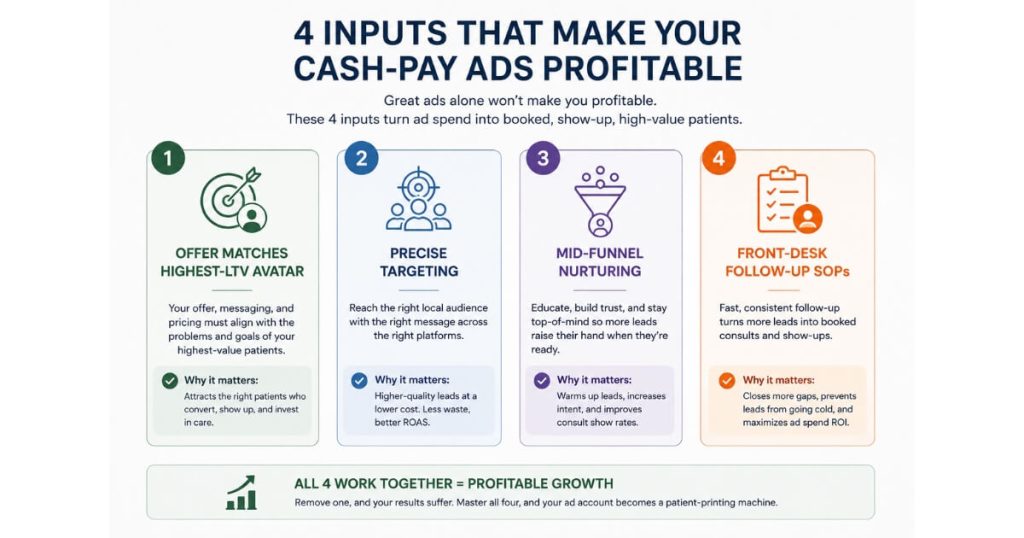
Most clinics that lose money on ads are not losing because the platform does not work. They are losing because one of those four inputs is broken.
We worked with an 11-location clinic across Arizona and Ohio that was spending on ads and losing money. The offer did not resonate with their most profitable patient type.
Once we ran the numbers and built the offer around the highest-lifetime-value avatar, they could spend three times more and still hold a strongly positive ROI.
We also worked with a clinic in Charlotte whose funnel was bleeding from the wrong targeting and zero nurturing.
We rebuilt it from the ground up with precise Facebook interest stacks, mid-funnel retargeting, a proven offer structure, and follow-up SOPs for the front desk.
Both clinics went from losing money to booking 20-plus qualified appointments a week. They became so successful that they are now booked out roughly two months because they cannot fulfill all the new demand.
A money pit is an account where the offer, targeting, nurturing, or follow-up is broken.
A profitable account is one where all four are dialed in.
We saw the same pattern at scale at NuLevel Wellness Medspa, where a multi-channel paid ad program drove $6.7M in one year across 3,727 new patients.
Why is lifetime value the number that actually determines your real ROAS?
Most cash-pay treatments recur or upsell. Because of that, first-purchase ROAS understates the truth.
The real return is the lifetime value of the patient divided by the cost to acquire them.
Clinics that build the offer around the highest-LTV avatar can profitably spend far more than clinics that optimize for the first sale.
When you know which patient type is worth the most over their full relationship with the clinic, you can afford a higher cost per acquisition on the front end. The back-end revenue carries it.
That is exactly what unlocked the three-times spend increase at the Arizona and Ohio clinic. Identifying the highest-lifetime-value avatar changed what a winning ROAS looked like overnight.
A clinic that measures only first-purchase ROAS will cap its spend too early. It will leave demand on the table. It will also watch competitors who understand LTV outbid them for the same patients.
Build the offer and the targeting around lifetime value. Then the ROAS math that looked break-even on day one becomes strongly profitable across the relationship.
What ROAS did Real ADvice’s case studies actually produce for cash-pay clinics?
The proof points are revenue at scale on paid ads, not theoretical benchmarks.
At NuLevel Wellness Medspa, a multi-channel paid ad program drove $6.7 million in revenue in one year across 3,727 new patients. It reached a run rate above $1 million per month.
That is what a dialed-in aesthetic and weight-loss stack produces when the offer, targeting, and follow-up are all in place.
At an orthopedic surgical center where we added $2M in revenue from Facebook ads alone, the result is what high-ticket cash-pay paid ads look like when the offer matches the avatar and the follow-up converts the lead fast.
Across three cash-pay clinics in a single year, we added $5 million in aggregate revenue by fixing the inputs that drive ROAS. Those inputs were the offer, the targeting, the nurturing, and the follow-up SOPs.
The realistic expectation is not a single ROAS multiple.
It is a profitable, scalable account where you can keep spending because the unit economics hold.
FAQ’s About Cash-Pay Clinic Paid Ad ROAS
Is a 3x ROAS good for a cash-pay medical practice?
A blended 3x ROAS on front-end revenue is a healthy, profitable result for most cash-pay clinics.
It usually understates the real return because the lifetime value of recurring and upsell revenue is not included in that first number.
For a low-ticket front-end offer, even a 1x to 2x ROAS can be the correct target. That is especially true when the offer exists to acquire the patient cheaply and earn on the back end.
Why is my clinic losing money on paid ads even though the platform should work?
It is almost always one of four broken inputs:
- The offer does not match your most profitable patient type.
- The targeting is too loose.
- There is no mid-funnel nurturing.
- The front desk has no follow-up SOPs to convert appointments into cash.
Fix those issues and the same ad spend that was losing money can turn strongly positive.
One clinic we worked with went from losing money to spending three times more at a positive ROI once the offer matched the highest-LTV avatar.
How fast should paid ads pay for themselves at a cash-pay clinic?
For most cash-pay offers, payback should land in days to a few weeks.
High-ticket front-end cash offers need cash to come in roughly as fast as you put it out. That only happens with fast follow-up.
Recurring care like TRT and HRT pays back within the first cycle or two. Everything after that is profit.
Should I optimize my ad account for first-purchase ROAS or lifetime value?
Optimize for lifetime value.
Most cash-pay treatments recur or upsell. Because of that, first-purchase ROAS understates the real return and caps your spend too early.
Building the offer around the highest-LTV avatar lets you afford a higher cost per acquisition. It also lets you outspend competitors who only count the first sale.
What ROAS should I expect on a high-ticket pain or neuropathy program?
A high-ticket program above $20K can realistically show a 4x to 8x ROAS on the very first sale.
The ticket absorbs the ad cost and still leaves margin.
However, this only works with a fast follow-up operation and a real sales process behind it.
Without that follow-up, the same offer becomes a money pit.
What’s the next step?
If you are spending on paid ads and the ROAS is not where it should be, the fix is rarely the platform.
It is the offer, the targeting, the nurturing, and the follow-up. These are the same four inputs that took an 11-location clinic from losing money to spending three times more at a positive ROI. They are also the same inputs that took a Charlotte clinic from a bleeding funnel to 20-plus qualified appointments a week.
Set your ROAS target by ticket and payback window.
Build the offer around your highest-LTV patient.
Make sure the cash comes in as fast as you spend.
If your cash-pay practice needs someone to audit the offer, the targeting, and the follow-up together and tell you exactly where the ROAS leak is, that is the conversation to book.
We will pull the numbers on your account on the call.