Does My Cash-Pay Medical Practice Need an HR Manager (And What That Role Owns)?
Most cash-pay clinic owners think HR is a big-company problem — until a bad hire, a compliance gap, or a wave of turnover costs them more than a year of marketing. The HR function isn’t paperwork. It’s the role that makes sure every office is properly staffed, every hire is onboarded and trained the same way, and your best people stay. Here’s the FAQ on what HR actually owns at a growing cash-pay practice, the non-negotiables you can’t skip, and when to make it a real role.
Does my cash-pay medical practice need an HR manager?
Yes — but it starts as a function before it becomes a full-time role.
Every clinic with employees already does HR. The only question is whether it’s done deliberately by someone who owns it, or accidentally by the owner between patients.
The HR function manages and performs the processes of recruiting, onboarding, training, and managing employees.
When a practice is small, the owner or office manager carries those tasks.
As you add providers, front desk, and coordinators across one or more locations, the volume and the risk both grow — and an unowned HR function is where bad hires, inconsistent training, and quiet turnover come from.
You make HR a dedicated role when the cost of getting people wrong exceeds the cost of the hire.
A growing cash-pay clinic with real recurring revenue cannot afford to staff by gut feel.
The same structural discipline that builds a medical practice marketing system that scales applies to people: define the role, document the process, and assign an owner.
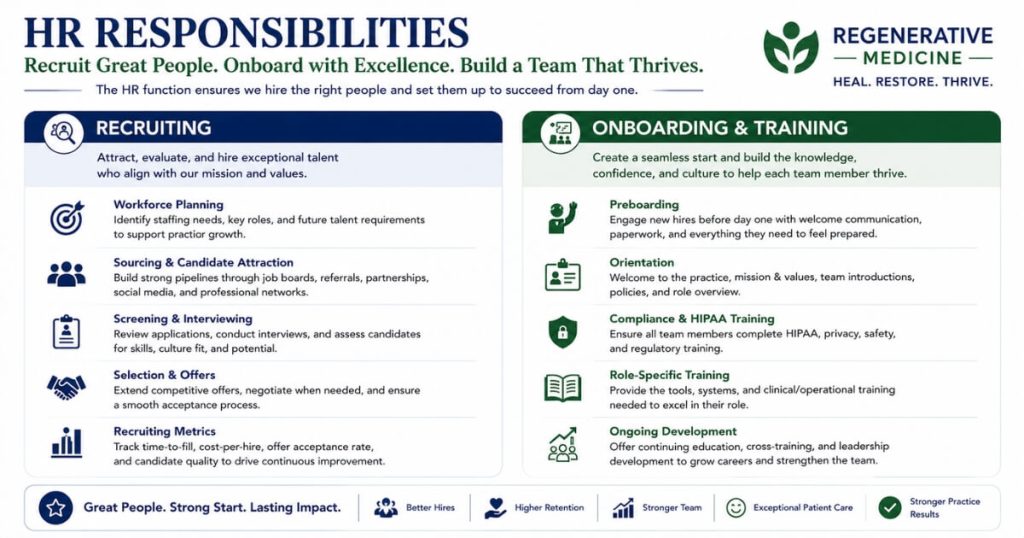
What does an HR manager actually do at a cash-pay clinic?
The HR manager is responsible for making sure all offices are properly staffed and managed, and that every employee is trained and onboarded according to your SOPs.
That breaks into two halves.
The first is recruiting:
- Sourcing and recruiting new employees
- Managing the recruitment process
- Candidate selection
- Scheduling and conducting interviews
- Running background checks
- Sending employment offer letters
- Collaborating with team managers on employee performance
The second is onboarding and people management:
- Sending welcome emails
- Creating personnel files
- Gathering personal documents
- Onboarding and training new employees
- Providing policies and procedures
- Running compliance training
- Managing the employee schedule
- Fielding time-off requests
- Finding coverage when needed
- Managing timesheets
- Making sure employees show up on time
Underneath all of it is one job that doesn’t fit on a task list: managing healthy, nurturing relationships with everyone on the team.
The HR manager is the person who keeps the culture drama-free and the staffing solid so the rest of the clinic can focus on patients.
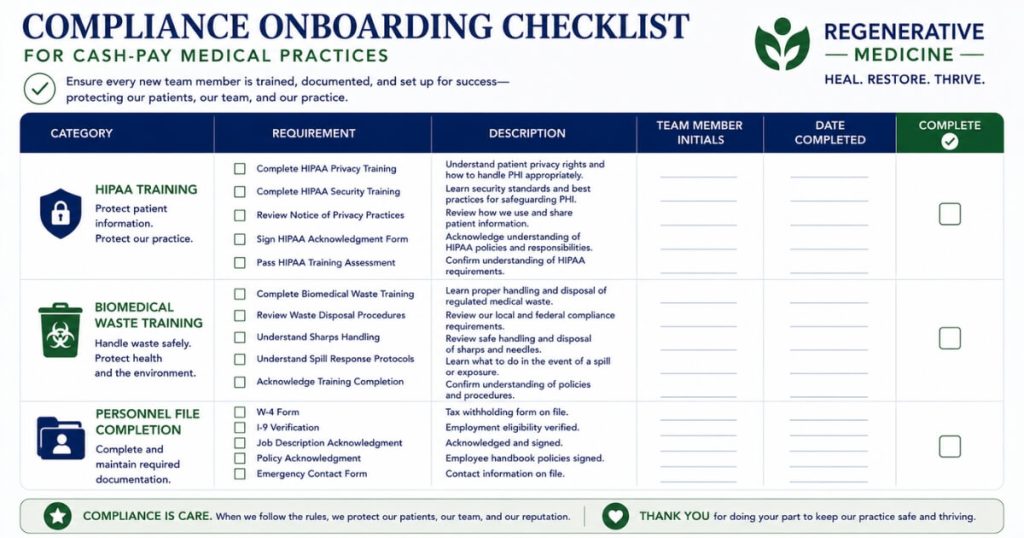
What HR tasks are non-negotiable for a medical practice?
Compliance onboarding — specifically HIPAA training and biomedical waste training — plus proper personnel files for every employee.
A marketing agency or a restaurant can be loose about onboarding.
A medical practice cannot.
Every new hire at a cash-pay clinic needs documented HIPAA training and, where applicable, biomedical waste training before they touch patient information or clinical materials.
Personnel files need to be created and complete, with personal documents gathered and policies and procedures formally provided and acknowledged.
These aren’t nice-to-haves; they’re the items that turn into real liability when they’re missing.
This is exactly why an unowned HR function is dangerous.
When onboarding is done ad hoc by whoever is free that day, compliance steps get skipped — not out of negligence, but because no one owns the checklist.
Assigning HR to one person, with a documented onboarding SOP, is how you make sure every hire goes through the same compliant process every time.
When should I hire an HR person vs keep it with the office manager?
Keep HR bundled with the office manager until hiring volume and headcount make it a job of its own — then split it out.
In the Real ADvice operational sequence, the office manager comes first and often carries HR early on.
That works while you’re hiring a few people a year.
The signal to split HR into its own role is when recruiting becomes continuous, when you’re staffing multiple locations, or when onboarding and people-management start eating so much of the office manager’s week that operations slip.
At that point HR is no longer a task — it’s a function that needs an owner, because every hour spent doing it well pays back in retention and every hour skipped shows up as turnover.
Getting this hire right is what lets owners genuinely scale out of the business.
Dr. Joy Kong hired four additional doctors and scaled herself out of the day-to-day of the clinic — a transition that only works when there’s a real people function recruiting, onboarding, and retaining the team behind the owner.
Likewise, Eternity Health Partners removed both owner-operators while growing from $1M to $4M a year, which is impossible without disciplined staffing underneath the growth.
If you’re weighing whether to build this in-house or get outside help, that’s a core question for the kind of medical practice marketing consultants who help owners structure the whole operation, not just the ads.
How do I measure whether my HR function is working?
By three outcomes: employee retention, performance, and satisfaction.
The HR role is judged on overall employee retention, performance, and satisfaction — not on how many interviews were scheduled or forms were filed.
Retention is the headline number:
A clinic that constantly re-hires the same roles is bleeding money and momentum, and that’s an HR signal before it’s anything else.
Performance tells you whether the people you hired and trained are actually moving the needle in their responsibilities.
Satisfaction tells you whether they’ll stay.
Track those three over time and you’ll know whether your people function is an asset or a gap.
When retention is high, performance is rising, and the team is satisfied, the rest of the clinic gets easier — the office manager isn’t constantly backfilling, the providers aren’t training a revolving door, and the owner isn’t pulled back into hiring every quarter.
FAQ’s About HR for a Cash-Pay Medical Practice
Can I outsource HR for my cash-pay clinic instead of hiring someone?
Yes, and many clinics start there.
A PEO or HR service can handle payroll, compliance, and benefits administration.
But sourcing, interviewing, onboarding, training, and the day-to-day relationship management still need an internal owner.
Outsourcing the paperwork doesn’t outsource the culture.
What’s the difference between the office manager and the HR manager?
The office manager runs the office day to day.
The HR manager owns the people pipeline — recruiting, onboarding, training, and retention.
In a small clinic one person does both.
As you grow, HR becomes its own role because hiring and retaining a team is a full-time job at scale.
What HR training is legally required at a medical practice?
HIPAA training is required for anyone who handles patient information, and biomedical waste training applies wherever clinical materials are handled.
Both should be part of a documented onboarding process completed before a new hire starts the relevant work, with the acknowledgment kept in the personnel file.
How do I reduce employee turnover at my clinic?
Treat retention as an HR outcome you measure, not an accident.
Consistent onboarding, clear policies, a drama-free culture, and real relationship management are what keep good people.
The clinics with the lowest turnover are the ones where someone actually owns retention as a number.
When is the right time to make HR a full-time role?
When recruiting is continuous, you’re staffing more than one location, or onboarding and people-management are crowding out operations for whoever currently carries it.
At that point the cost of doing HR poorly — turnover and compliance risk — exceeds the cost of a dedicated hire.
What’s the next step?
If your cash-pay practice is growing and you’re feeling the pain of inconsistent hiring, skipped onboarding steps, or turnover you can’t explain, the fix is structural: define the people function, document the process, and decide who owns it.
On a 60-minute strategy call we’ll map your org structure, show you where HR should live today versus after your next growth stage, and help you build the recruiting and onboarding system that keeps your team solid as you scale.