Why Speed to Lead Matters More Than Follow-Up Volume at a Cash-Pay Medical Practice (The 5-Minute Rule That Decides Whether They Pick Up)
Most cash-pay clinics over-invest in follow-up automation and under-invest in initial-response staffing — and wonder why their conversion rate is stuck.
Speed-to-lead is the single highest-leverage sales metric a cash-pay medical practice can control. It is also the cheapest to fix.
The first 5 minutes after a form submission, a deposit payment, or an inbound call is the window when the patient’s motivation is at peak, the phone is still in their hand, and they will answer when you ring.
Wait 6 hours and the same lead has gone cold — not because they changed their mind, but because emotional decay closed the window.
This is the FAQ on the 5-minute rule, why it works for weight loss / HRT / regen / longevity, and the staffing math behind making it actually happen.
How Fast Should a Cash-Pay Medical Practice Call Back a New Lead?
Inside 5 minutes of the lead form submission, deposit payment, or inbound call.
Anything slower than 5 minutes and the connect rate collapses by half.
Anything slower than 24 hours and the lead is functionally dead.
Why Does This Happen?
The reason is not laziness or short attention spans — it is emotional decay.
A cash-pay medical practice patient inquires when they are at the peak of motivation.
They are fed up with the symptom, they have decided to act, and they have just filled out the form.
That emotional spike fades fast.
The phone they were holding three minutes ago is now in their pocket.
The text they were going to read is now buried under three new ones.
The motivation that drove them to submit the form is gone within the hour.
The clinic that calls inside 5 minutes catches them on the emotional spike.
The clinic that calls the next morning catches them at zero.
Same lead. Different outcome.
Speed-to-lead is the single highest-leverage sales metric a cash-pay clinic can control.
Why Does Emotional Decay Make Speed-to-Lead the Most Important Conversion Metric for Cash-Pay Medicine?
Because cash-pay medicine treats conditions where the patient is emotionally driven, not clinically referred.
The Decision Is Made in Minutes, Not Days
Weight loss is emotional.
Hormone replacement is emotional.
Regenerative pain treatment is emotional.
Longevity is emotional.
The patient is paying out of pocket because they have hit a wall — the way they look in the mirror, the energy drop in the afternoon, the joint pain on stairs, the perimenopause symptoms nobody warned them about.
The decision to act on that is made in a window of minutes, not days.
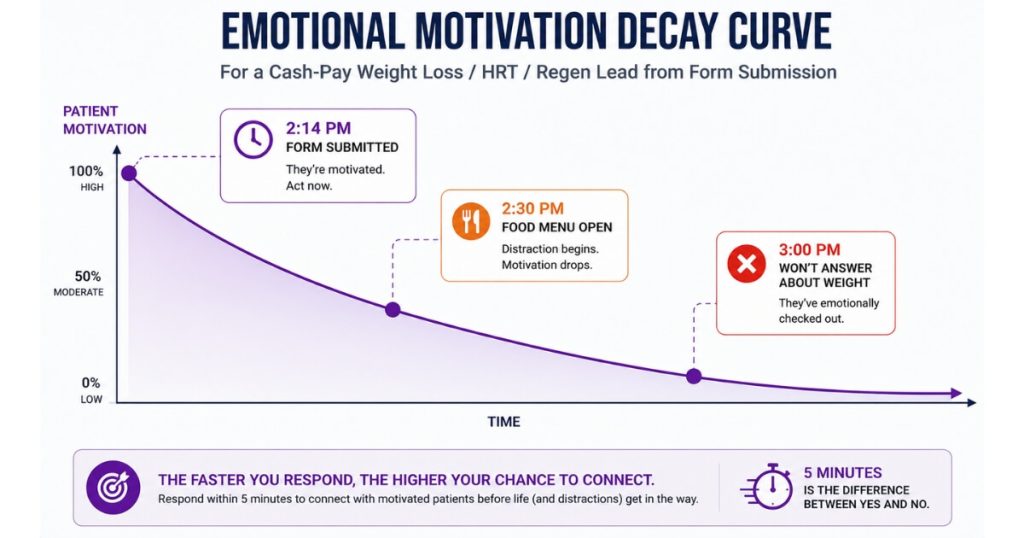
A weight loss patient who fills out a form at 2:14 PM is fed up at 2:14 PM.
By 2:30 PM the food delivery menu is open and the resolve is gone.
By 3:00 PM they are not going to answer the phone because they do not want to have a conversation about their weight.
Speed-to-lead is not a phone metric.
It is an emotion-window metric.
The clinics that understand this staff for it.
The clinics that do not see the emotion close before they ever pick up the dial.
What’s a Realistic Speed-to-Lead Benchmark for a Cash-Pay Medical Practice?
Benchmark Targets
- Top quartile: median 90 seconds, 90th percentile under 5 minutes
- Acceptable: median 4 minutes, 90th percentile under 15 minutes
- Below acceptable: median 30+ minutes or any leads sitting overnight
The number that matters is the 90th percentile, not the average, because the average hides the leads that sat for 6 hours and ruins the conversion math for the leads that got called fast.
Most cash-pay clinics underestimate their speed-to-lead because they measure it from the perspective of “we always call the same day.”
The clinic that calls a 9:00 AM lead at 4:30 PM technically called the same day — and the lead is dead by 4:30 PM.
How Should You Measure Speed-to-Lead?
The right unit of measurement is minutes from form submission to the first dial, every single time, with the 90th percentile reported weekly.
Most cash-pay clinics that install the metric see it drop from 90 minutes to under 10 minutes inside 60 days, with a measurable conversion lift the same quarter.
A regenerative medicine clinic we worked with hit a 79.4 percent conversion rate from lead to booked appointment by installing exactly this discipline at the front desk.
How Does a Cash-Pay Clinic Actually Staff for Sub-5-Minute Speed to Lead?
Three options, in order of cost and reliability.
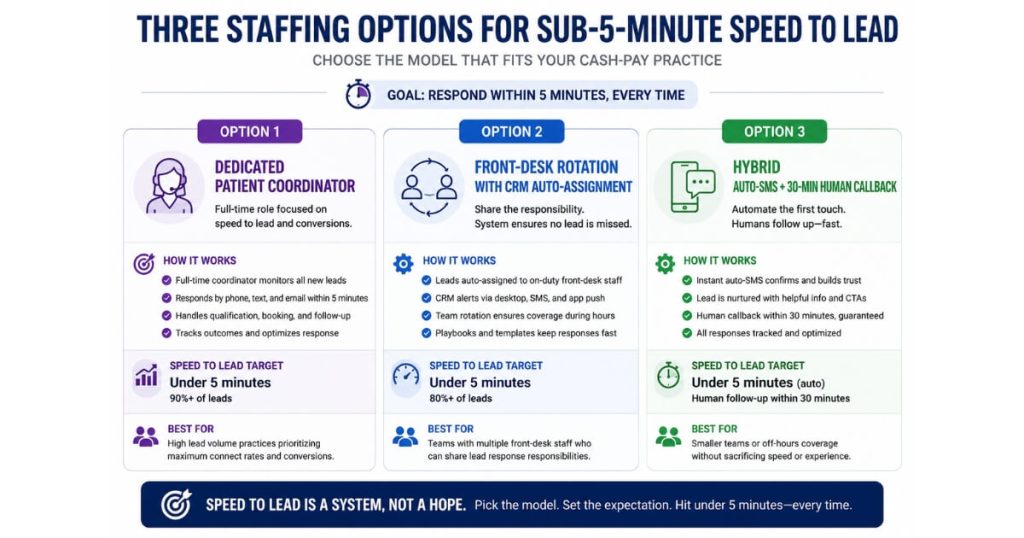
Option One
A dedicated patient coordinator whose only job during business hours is responding to new leads and inbound calls.
This is the cleanest solution for clinics doing $1M+ revenue.
Option Two
A rotation of front-desk staff with explicit lead-response coverage on a daily schedule, paired with a CRM that auto-assigns the lead to whoever is on shift.
This works for clinics in the $300K-$1M band.
Option Three
A hybrid where automated SMS and email respond inside 60 seconds with a personal touch, and the human callback happens inside 30 minutes.
The auto-response buys the clinic 25 minutes of emotional bridge while a human gets free.
What Happens After Hours?
After hours, the auto-response sets expectations (“a team member will call you at 8:00 AM tomorrow morning, mark it in your calendar”) and the morning queue is the first thing that hits the phone.
The mistake is leaving lead response as an undefined “whoever picks it up first” responsibility.
That is how a 5-minute lead becomes a 6-hour lead, and a 70% connect rate becomes a 30% connect rate.
What About Leads Who Paid a $50 Deposit but Won’t Answer the Phone — Why Does That Happen?
Because the deposit was the easiest part of the decision and the conversation is the hardest part.
A $50 deposit on a weight loss consult feels like an investment in a future self.
A phone call about that weight loss consult feels like a confrontation with the present self.
Patients who pay deposits and then go dark are not unmotivated buyers — they are buyers whose motivation flickered the moment the cost of action shifted from a click to a conversation.
The Real Issue
The fix is the same as for any other speed-to-lead problem: call them faster, inside the emotion window, before the embarrassment kicks in.
Clinics that see “paid deposit, won’t respond” patterns across more than 20% of deposit leads have a speed problem that the deposit cannot solve.
The deposit is a commitment device; it is not a substitute for catching the patient in the emotion that drove the deposit.
Three contact attempts across two days, then move the lead to “abandoned” — that is the standard pursuit window.
After two days the lead is cold and forcing more dials does more damage than good.
Should a Cash-Pay Clinic Prioritize Speed-to-Lead Over Follow-Up Volume?
Yes.
Speed beats volume at every comparable budget.
A clinic that calls 100 leads inside 5 minutes books more consults than a clinic that calls the same 100 leads 10 times each over 14 days.
The asymmetry is large enough that most cash-pay clinics over-invest in follow-up automation and under-invest in initial-response staffing — and they wonder why their conversion rate is stuck.
The Right Order
The right sequence is speed first, then volume.
The first 5 minutes captures the patients who were ready to talk.
The follow-up cadence captures the patients who were ready to talk but couldn’t pick up in that moment.
Follow-up volume cannot rescue a lead that went cold because nobody called in time.
A 21-touch cadence on a 6-hour-old lead has a fraction of the conversion rate of a single touch on a 5-minute-old lead.
This is the practical impact of the 5-minute speed-to-lead rule. The goal is not to overwhelm prospects with more calls, texts, and emails — it’s to reach them while their motivation is still at its highest point. Clinics that consistently connect with new inquiries within minutes create more conversations, book more appointments, and generate more revenue without increasing lead volume or advertising spend.
Spend the marketing dollar on the team that picks up the phone, not on the third SMS in a multi-day drip.
An HRT clinic we grew from $1M to $4M in 4 years built its book of business on this exact discipline — speed first, structured follow-up second.
What’s the Next Step?
If your cash-pay clinic has never measured speed-to-lead at the 90th percentile level — or you suspect that “we always call the same day” is hiding a 4-hour median that is costing you 20-30% of your potential conversions — the audit and fix is the most efficient sales improvement available.
What Happens on the Call?
On the call we pull the speed-to-lead distribution from the last 90 days (median, 90th percentile, after-hours percentage), audit the lead-response staffing model, and design the patient coordinator coverage schedule, the CRM auto-assignment rules, and the auto-response SMS template.
The implementation usually takes 30-60 days to install end-to-end and produces a measurable conversion lift in the same quarter.
Speed-to-lead is the single fastest cash-pay sales improvement available because the levers are operational, not creative — no new copy, no new offer, no new platform, just a faster phone.