What Is the Right Price for a PRP, Stem Cell, or Exosome Treatment at a Cash-Pay Regenerative Medicine Clinic?
Pricing is the single most under-engineered variable at most cash-pay regenerative medicine clinics. The clinic with the right protocol, the right provider, and the right inside-sales seat still loses revenue if the price is built from the cost of the inputs rather than from the value of the outcome. The clinic that nails the protocol-package-financing structure converts at multiples of the clinic running line-item pricing on the exact same procedure menu. Here is the FAQ on how cash-pay regen clinics actually price PRP, stem cell, and exosome protocols — what each tier costs, how to package, when to offer financing, and how pricing structure changes conversion.
What is the right price for a PRP, stem cell, or exosome treatment at a cash-pay regenerative medicine clinic?
Realistic pricing across cash-pay regen clinics in 2026
Realistic pricing across cash-pay regen clinics in 2026:
- a standalone PRP single-joint procedure prices around $750 per joint
- a standalone stem cell or exosome single-joint procedure prices $4,000–$6,000 per joint
- a packaged 12-week protocol (3 injection visits + imaging + follow-ups + recovery support) prices $10,000–$15,000
- multi-joint packaged protocols price $15,000–$25,000+
- systemic / IV / executive longevity programs price $25,000–$50,000+
The most important gap in regen pricing
The single most important number in that list is not any of the individual tiers — it is the gap between the $750 standalone PRP commodity injection and the $12,500 packaged 12-week regenerative program.
Same provider.
Same core therapeutic.
Dramatically different patient experience, dramatically different revenue per case.
Understanding pricing PRP, stem cell, and exosome treatments correctly is what allows regenerative clinics to move from selling individual procedures to selling comprehensive treatment programs that better reflect the value of the outcome patients are seeking.
That gap is the entire thesis of regen pricing.
What patients actually pay for
Patients pay for the program:
- the imaging baseline
- the multi-visit treatment arc
- the provider check-ins
- the recovery support
- the structured follow-up
They do not pay for the vial of PRP.
What changes the pricing range
The wide ranges inside each tier reflect three real variables:
- geography (a clinic in a major metro with high cost of living and high-disposable-income patients prices at the top of the range; a clinic in a smaller market prices in the middle)
- provider reputation (a board-certified specialist with published outcomes prices at a premium to a clinic where the provider is less known)
- protocol complexity (a single injection is dramatically different from a 12-week joint restoration program with three treatments, imaging, and follow-up visits)
Pricing inside those ranges should reflect the actual program the clinic delivers — patients pay for the program experience, not the cellular product cost.
The core pricing principle
The principle underneath every successful regen pricing structure:
- price the outcome
- package the program
- anchor the value
- never let the patient see the inputs
A clinic that publishes “$750 per PRP injection” on its website has set a ceiling on its own revenue and turned itself into a commodity vendor competing on price.
A clinic that publishes “12-week knee restoration program — $12,500, includes imaging review, three injection visits, two follow-up consults, and a one-year recovery membership credit” has anchored value, removed the negotiation surface, and signaled clinical depth.
Same provider, same procedure menu, dramatically different patient experience and revenue per case.
How do you price a standalone procedure vs. a packaged program vs. a multi-joint or systemic protocol?
The pricing ladder
Standalone PRP at the commodity tier (~$750 per joint), standalone stem cell or exosome at the premium single-joint tier ($4,000–$6,000), packaged 12-week protocols as the core revenue tier ($10,000–$15,000), multi-joint packages as the compounding tier ($15,000–$25,000+), and systemic / executive longevity as the high-LTV tier ($25,000–$50,000+).
Standalone PRP single-joint procedures
The Standalone PRP single-joint procedures sit at the commodity end of the market at ~$750 per joint.
This tier exists because the patient population that walks in asking for “just a PRP injection” is shopping on price and has often researched the procedure independently.
Clinics that price competitively at this tier use it as a lead-generation entry — a patient who books a single PRP injection often comes back six weeks later for a packaged program when the standalone injection alone did not produce the durability they wanted.
Treat the commodity tier as the door, not the destination.
Standalone stem cell or exosome single-joint procedures
Standalone stem cell or exosome single-joint procedures price at $4,000–$6,000 per joint.
Patients in this tier are not price-shopping the way PRP patients are — they have researched the cellular product, they understand it is a different therapeutic class, and they have already decided the higher price is justified.
Standalone pricing here makes sense when the clinic does not have a fully developed packaged program yet, but most clinics convert these patients into packaged programs at the consult because the unit economics on the program are dramatically better.
Packaged 12-week protocol
The packaged 12-week protocol is the core revenue tier and where most cash-pay regen clinics should be focused.
Three injection visits, imaging baseline, two follow-up consults, recovery support, and a one-year recovery membership credit — $10,000–$15,000 depending on cellular product, geography, and positioning.
Patients new to the practice book this tier most often when the consult is run cleanly, because the program is comparable to surgery they want to avoid — not to a $750 commodity injection.
Multi-joint tier
The multi-joint tier is where revenue per case compounds.
A patient with knee and hip pain pays for the knee protocol at $12,500 and the hip add-on at roughly half — $6,000–$7,000.
The total package lands at $18,500–$19,500, the patient gets a more comprehensive treatment plan, and the clinic captures more revenue per consult-hour spent.
Second-joint discount logic
The discount logic on the second joint is critical:
- full price on every joint feels punitive
- full price on the first plus a meaningful discount on additional joints feels like a fair package
Patients pay readily for the second number; they push back on the first arithmetic.
Systemic tier
The systemic tier is where the highest-LTV patients live.
Executive longevity programs ranging $25,000–$50,000+ cover:
- IV stem cell or exosome infusions
- ongoing peptide protocols (where legally permitted)
- hormone optimization
- full lab panels
- body composition tracking
- a 12-month membership of provider access
This tier converts less often per consult but produces dramatically higher revenue per converted patient, and these patients refer at higher rates than any other segment.
The patient population that buys this tier is the same one that drove Eternity Health Partners’ growth from $1M/year to $4M/year over four years through high-LTV membership programs — different specialty, same patient psychographic.
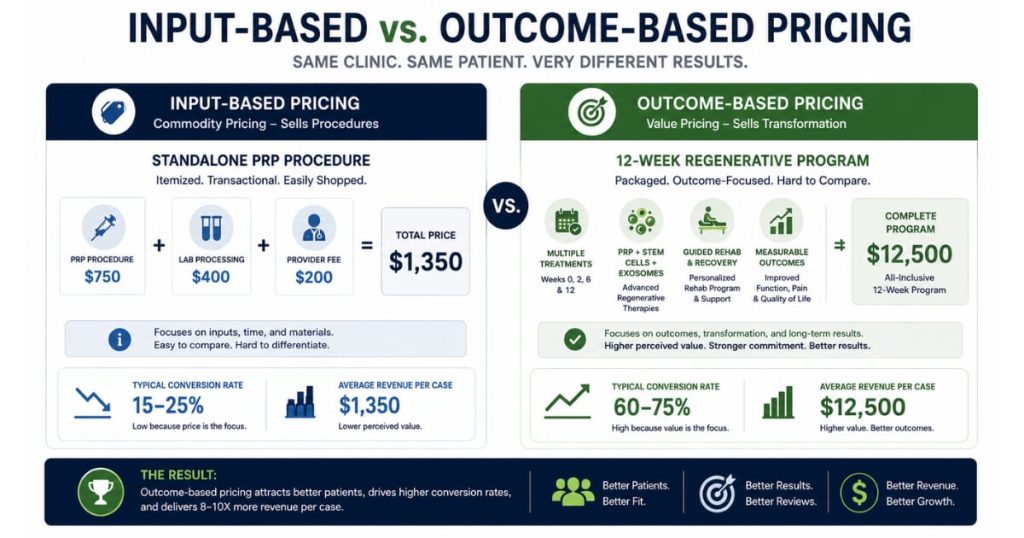
What’s the difference between input-based pricing and outcome-based pricing — and why does it matter?
Input-based pricing
Input-based pricing builds the patient-facing price from the cost of materials and provider time — a $200 vial of PRP plus a 45-minute provider block plus disposables equals a $750 commodity procedure.
Outcome-based pricing
Outcome-based pricing builds the price from the value of the clinical result — what is it worth to a 58-year-old to delay a knee replacement by five years — and arrives at a $10K–$15K packaged program with no change in inputs.
The first problem with input-based pricing
The first problem with input-based pricing is that it sets a ceiling defined by the patient’s perception of cost rather than their perception of value.
A patient who is told their $750 PRP injection includes “the vial, the provider time, and the equipment” mentally adds up those line items and decides whether $750 sounds like a fair markup.
The conversation is now a transaction.
A patient who is told their $12,500 12-week knee restoration program includes “imaging, three injection visits, two follow-up consults, and a one-year recovery membership credit” is not adding up inputs — they are evaluating the program.
The price feels expensive in absolute terms but reasonable relative to the alternative (surgery they want to avoid).
Same provider, same actual product, dramatically different patient framing.
The second problem with input-based pricing
The second problem with input-based pricing is that it makes the practice the seller of a product and the patient the buyer of an input.
Once that frame is set, the patient negotiates on the input cost.
“Can you do it for $600?” is a question that arrives when the price is presented as the sum of components.
“Can you do it for $11,000 instead of $12,500?” almost never arrives when the price is presented as a program — patients negotiate on transactions, not on programs.
The third problem with input-based pricing
The third problem is operational.
Input-based pricing requires the provider to defend the margin every time the cost of materials changes.
Outcome-based pricing absorbs material cost variance inside the program price — the provider does not have to reprice when the supplier raises rates, because the program price was never built off the supplier rate in the first place.
Why outcome-based pricing wins
The clinics running 60–80% lead-to-booked conversion rates almost universally use outcome-based program pricing.
The clinics stuck at 20–30% almost universally use input-based itemized pricing.
This is not coincidence — it is the patient experiencing the same procedure as a program in one clinic and a transaction in the other.
The 79.4% conversion rate at Orthobiologics Associates ($309,590 in cash-pay revenue in 10 months from organic search with zero ad spend) sat on top of a packaged-program pricing structure, not a per-injection price list.
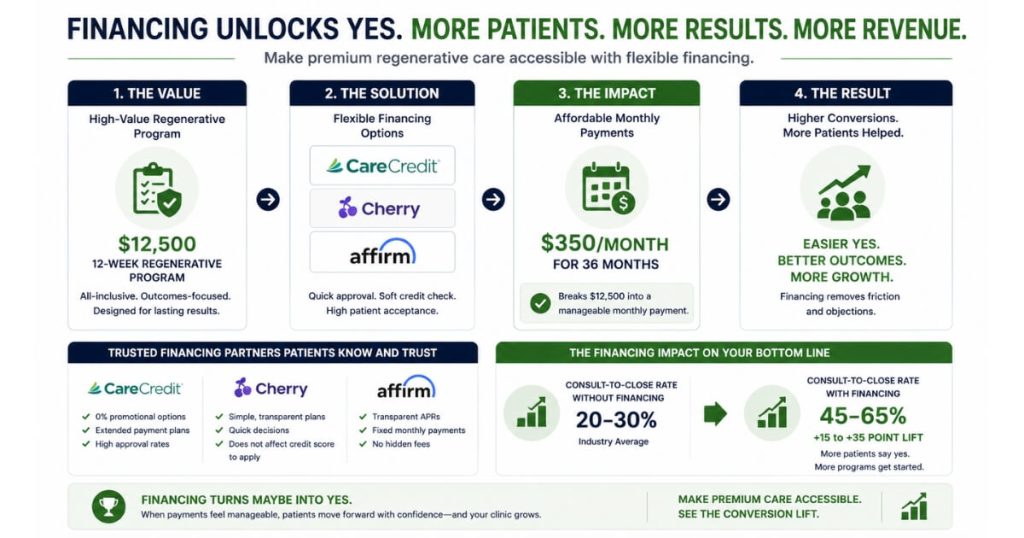
Should a cash-pay regenerative medicine clinic offer financing? Does it lift or hurt conversion rate?
The short answer
Yes, financing lifts conversion rate when offered correctly — but it has to come into the conversation at the right moment, never as the lead, and never as the answer to a price objection.
The financing math
The math:
- a regen clinic offering CareCredit, Cherry, or Affirm at the consult lifts close rate by 15–30 percentage points for packaged programs above $5,000
- the patient who would have walked away from a $12,500 lump sum says yes to roughly $350/month for 36 months
- same patient, same protocol, same revenue to the clinic (because the clinic gets paid by the financing company up front, minus a fee)
- the financing partner absorbs the patient credit risk in exchange for a 4–12% transaction fee depending on the program and the patient’s credit profile
The timing matters more than the financing partner.
The correct sequence
- Present the program.
- Present the price.
- Let the patient sit with both.
If the patient says yes, you do not mention financing — collect payment in full or set up the payment plan they chose.
If the patient hesitates and the hesitation appears to be a payment-mechanics question rather than a program-fit question, that is the moment to introduce financing as the bridge.
“Many of our patients use a 36-month financing option for this program — would that change the timing for you?”
The wrong sequence
The wrong sequence is leading with financing.
“We have financing available starting at $350/month” in the ad copy or on the landing page anchors the patient on the monthly payment and destroys the program-pricing frame.
Patients arrive at the consult thinking they are buying a $350/month subscription and walk out when they discover the actual total.
Financing is a bridge, not a hook.
The hook is the program value; the bridge gets the patient across once they have already decided the program is right for them.
Two financing mistakes clinics make
The clinics that miscalculate financing tend to do so in two ways.
The first
The first is using financing as the answer to every objection — which trains the Patient Coordinator to skip the program qualification step and go straight to “we have financing.”
The second
The second is offering only one financing partner, which means patients denied by that one partner have no alternative.
Best practice
Best practice:
- two financing partners in the stack (typically one mid-prime and one near-prime)
- used only when the patient has decided to enroll and the only question is mechanics of payment
How does package pricing change the consult-to-procedure close rate?
Package pricing lift
Package pricing typically lifts consult-to-procedure close rate from 25–35% (on itemized pricing) into the 55–75% range, and lifts average revenue per closed case by 4–8× — because the package both increases the patient’s perceived value and removes the per-line-item negotiation surface.
The patient’s decision architecture
The mechanism is not about the math; it is about the patient’s decision architecture.
A patient evaluating an itemized regen quote — “$750 PRP injection, $400 imaging, $200 follow-up, total $1,350” — is making three separate decisions and looking for cuts at every line.
The clinic is also implicitly inviting that negotiation by having presented the price that way.
The same patient evaluating a packaged program — “12-week knee restoration protocol, $12,500, includes everything we just discussed” — is making one decision:
- do I want this program or not
The negotiation surface is gone.
The patient either says yes or no to the whole thing.
The all-in program
The packaging move that produces the biggest single conversion lift is what we call the “all-in program” — every reasonable adjacent service rolled into the main price so the patient is never surprised by a follow-on charge.
Imaging review, baseline assessments, three injection visits, two follow-up consults, recovery protocols, and a small membership credit for the first 12 months.
All inside the program price.
Patients pay readily for “everything you need for 12 months, included” — they push back hard when the consult ends with a price they thought was the total and a stack of “and these are extra” line items.
Two effects from packaging
The clinics that have made this packaging move see two parallel effects.
First
First, close rate rises immediately — patients accept the program where they previously walked away from the line items.
Second
Second, average revenue per case rises substantially because the same provider, the same procedure, and the same chair-time now generates the price of a real program rather than the price of a commodity injection.
A clinic doing standalone PRP at $750 per injection makes a fraction of what the same clinic makes the day it shifts to packaged 12-week protocols at $12,500 — even with a higher absolute price, conversion improves because the patient is finally being offered something proportional to the result they want.
How should pricing flex by geography, provider reputation, and clinic positioning?
The three pricing levers
Geography moves prices 20–40% across major US markets.
Provider reputation moves prices 30–80% within the same market.
Clinic positioning (premium concierge vs. accessible boutique) moves prices another 20–50% on top of geography and reputation.
Geography
Geography is the easiest variable to calibrate.
A regen clinic in San Francisco, Los Angeles, Manhattan, Miami, or Austin can defensibly price 20–40% above a comparable clinic in a smaller US market because patient income, cost of living, and price expectations all run higher.
The mistake clinics make in higher-cost markets is failing to price at the market rate because the owner is anchored on what they would pay personally — pricing for the avatar that actually books, not for the owner’s own price tolerance, lifts revenue meaningfully.
Provider reputation
Provider reputation is the variable most owners under-price.
A board-certified physiatrist with published outcomes, a faculty appointment, or 10+ years of specialty practice can price 30–80% above a clinic where the provider is less known — and patients pay readily because the price increase is interpreted as a signal of clinical quality.
The mistake here is the provider’s personal humility undercutting the practice’s revenue.
The provider does not have to feel comfortable with the higher price; the practice has to set it.
Clinic positioning
Clinic positioning is the variable most strategically deployable.
A “premium concierge” position (low patient volume, high touch, dedicated provider time, white-glove logistics, $25,000+ programs) plays a different game than an “accessible boutique” position (higher patient volume, structured intake, defined protocol menus, $10,000–$15,000 programs).
Both can be profitable; both serve different patient segments.
The mistake is trying to be both at the same time — running a high-touch concierge experience while pricing at boutique levels, or pricing at concierge levels with boutique operational infrastructure.
The two positions converge nowhere; pick one cleanly.
The regen pricing meta-rule
The pricing-strategy meta-rule for regen clinics:
- price the upper end of what your geography, provider, and positioning can defensibly support
- then deliver an experience that makes the price feel right at the consult
Under-pricing is reversible but never advisable in cash-pay medicine; over-pricing within a defensible range is recoverable through delivery quality.
The clinics that grow fastest tend to be the ones that priced confidently at the top of their defensible range from day one.
What’s the next step?
If you run a cash-pay regenerative medicine clinic and your conversion rate is sitting below 50%, the pricing structure is one of the three variables that fix it (along with the inside-sales seat and the speed-to-lead operational layer).
Move from itemized pricing to packaged programs.
Move from input-based math to outcome-anchored value.
Layer in financing at the right consult moment.
Calibrate the range to your geography, provider, and positioning rather than to your own price tolerance.
If you want a 60-minute walk-through of where your current pricing structure is leaving revenue on the table, what your packaged-program prices should be by protocol type, and how to introduce financing without anchoring patients to a monthly-payment frame, book a strategy call.
We will pull your current price list and your consult conversion data on the call.