What Conversion Rate Should a Cash-Pay Regenerative Medicine Clinic Aim For? (And How Orthobiologics Hit 79.4%)
Most cash-pay regenerative medicine clinics convert somewhere between 15% and 25% of leads into booked, paid consults. The clinics actually growing — the ones doing $300K, $500K, $1M+ a year in cash-pay revenue without burning the owner out on paid ads — convert 60% to 80%. The difference is not the lead source. It is what happens in the 90 seconds after the phone rings, the 24 hours after the form gets filled out, and the discovery-call structure that follows. Here is the FAQ on what conversion rate to aim for at a cash-pay regen clinic, where most clinics leak patients, and the inside-sales playbook one of our clients used to hit 79.4%.
——————————————————————————
What conversion rate should a cash-pay regenerative medicine clinic aim for?
The realistic target is 60% to 80% from inquiry to booked, paid consult. Industry average is 15% to 25%. The gap is operational, not market-driven.
A 60–80% lead-to-booked rate is what cash-pay regen clinics with a working inside-sales seat actually produce.
What the numbers usually mean
- Below 30% means the front desk is treating regen inquiries like insurance bookings — taking a message, sending a callback.
- Below 50% means the clinic has a salesperson but no qualification framework, so the wrong patients get booked and the right patients ghost.
- Above 60% means there is a Patient Coordinator running a written process:
- speed to lead
- qualification on the first call
- a clear value frame for the $7K–$15K procedure
- a credit-card hold or paid consult as the close mechanism
The industry average sits at 15–25% because most regenerative medicine clinics still run the front desk as a receptionist role.
A patient calls asking about stem cell injections, the front desk says:
“let me have one of our coordinators call you back”
—and 80% of those callbacks never connect.
The leads that came in cold from:
- a Facebook ad
- a Google search
needed a human voice inside two minutes, not two hours.
Every minute past the first 60 cuts the booking rate roughly in half.
By the third day, the lead is functionally dead.
Orthobiologics Associates hit 79.4%.
The case study has the receipt — $309,590 in cash-pay revenue in 10 months from SEO leads only, no paid ads.
The structural change underneath that number is what this FAQ is about.
——————————————————————————
How did Orthobiologics Associates hit a 79.4% conversion rate without paid ads?
By installing the Real ADvice Inside Sales 4 R’s framework into the Patient Coordinator role, then running every regen inquiry through the same documented process — every time.
The 4 R’s framework
- Roles
- Responsibilities
- Reporting
- Results
The framework defines:
- what the Patient Coordinator owns
- who they report to
- the metrics they hit weekly
- the consequences for missing those metrics
At Orthobiologics, the Patient Coordinator was responsible for:
- Answering every regen inquiry inside 5 minutes of the lead landing.
- Qualifying the patient on the first call against a written checklist:
- presenting condition
- prior treatments
- pain level
- urgency
- financial readiness
- Scheduling the paid consult on the same call.
- Capturing payment for the consult before hanging up.
Reporting cadence
- Daily call logs reviewed Friday.
- Conversion rate posted on the team dashboard.
- Written explanation required for any week below 60%.
Results measured
- Conversion rate.
- Number of paid consults booked per week.
The Orthobiologics Associates case study covers the rest in detail — $309,590 in cash-pay revenue in 10 months, 79.4% lead-to-booked conversion, all from organic search, with zero ad spend.
The reason it scaled without a paid-ads budget is that conversion rate compounded the value of every SEO lead — when 79 out of every 100 leads booked, the clinic did not need to feed the funnel with paid traffic.
They needed to protect the inside-sales seat.
The mistake clinics make trying to copy this is hiring:
“a great front desk lead”
and calling them a Patient Coordinator.
The title is not the system.
Without the 4 R’s structure — and specifically without the weekly results review — the role drifts back into receptionist work within a quarter.
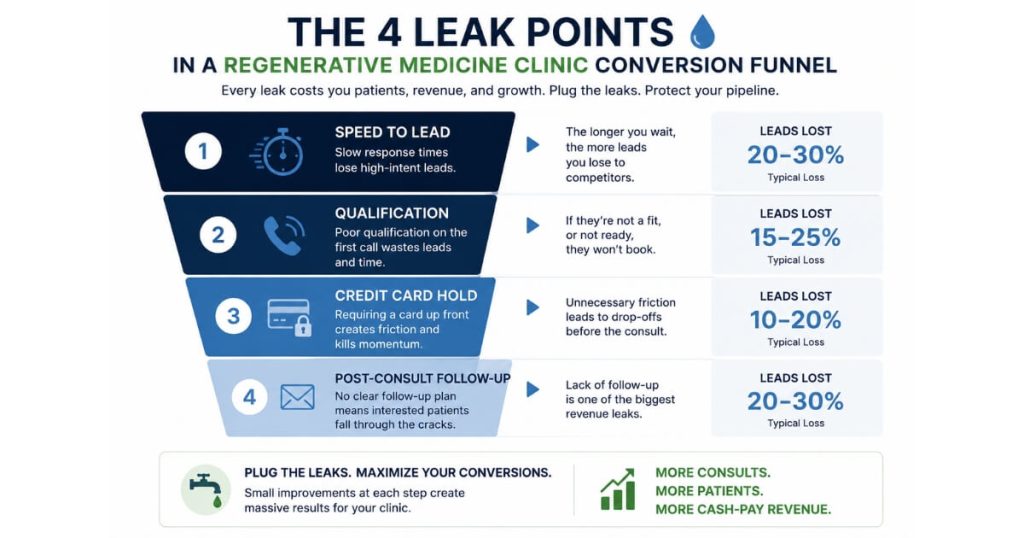
Where do regenerative medicine clinics actually lose patients between the inquiry and the consult?
Four leak points, in this order:
- Speed to lead
- Qualification on the first call
- The credit-card hold for the consult
- The 24-hour follow-up after the consult
1. Speed to lead
Speed to lead is the biggest leak by a wide margin.
A regen patient calling about a $10K procedure is:
- in pain
- scared
- shopping
They are calling two or three clinics that afternoon.
The first clinic that picks up usually books the consult.
Most regen clinics route inquiries to a callback queue and lose half of them inside an hour.
The fix:
- Real human answering inside 5 minutes during business hours.
- Automated SMS plus voice callback inside 15 minutes after hours.
No exceptions.
2. Qualification on the first call
Most clinics ask:
“what insurance do you have”
and lose the patient on the first sentence because the patient knows they have no insurance coverage for regen.
The correct first questions are about:
- the condition
- prior treatments tried
- pain level
- urgency
The Patient Coordinator is not selling on the call.
They are figuring out whether the patient is ready to invest in a self-pay procedure and, if so, getting them on the calendar.
3. Credit-card hold for the consult
Some clinics use a credit-card hold.
Others use a $300–$500 paid consult.
Patients who book a free consult no-show at 30–50%.
Patients who put a credit card down for the consult no-show at single digits.
This is not about gating access.
It is about filtering for intent.
4. 24-hour follow-up after the consult
The provider does a great consult.
The patient leaves to:
“think about it”
The clinic never calls back.
The Patient Coordinator’s job is:
- same-day text recapping the protocol
- next-day call discussing financing options if needed
- third-day check-in if the procedure hasn’t been booked
Most conversions happen on follow-up call two or three.
Clinics that do not run a structured follow-up sequence leave 30–40% of booked-procedure revenue on the table.
——————————————————————————
Should a cash-pay regenerative medicine clinic track cost per lead or conversion rate first?
Conversion rate first. Always.
Cost per lead is meaningless until conversion rate is fixed.
Example
A regen clinic with:
- 20% conversion rate
- $50 cost per lead
is paying:
- $250 per booked consult
The same clinic at:
- 60% conversion
is paying:
- $83 per booked consult
Three times the efficiency on the same ad spend.
Why conversion rate comes first
- Cutting CPL through ad optimization is usually a 5–15% win.
- Doubling or tripling conversion rate is a 100–300% win.
Fix conversion first.
Then optimize lead cost.
Before increasing ad spend, every clinic should understand the conversion rate a regenerative clinic should aim for, because improving lead-to-consult conversion often produces a larger revenue gain than lowering cost per lead.
This is also why so many regenerative medicine clinics conclude that paid ads:
“don’t work”
They tested Facebook or Google with a broken funnel underneath, watched CPL look fine while booked-consult rate was 18%, and blamed the channel.
The channel was not the problem.
The conversion engine was.
Correct order of operations
- Install the Patient Coordinator seat with the 4 R’s framework.
- Get conversion rate above 50% on existing organic flow.
- Document the qualification script.
- Document the consult-follow-up sequence.
- Then turn on paid ads.
——————————————————————————
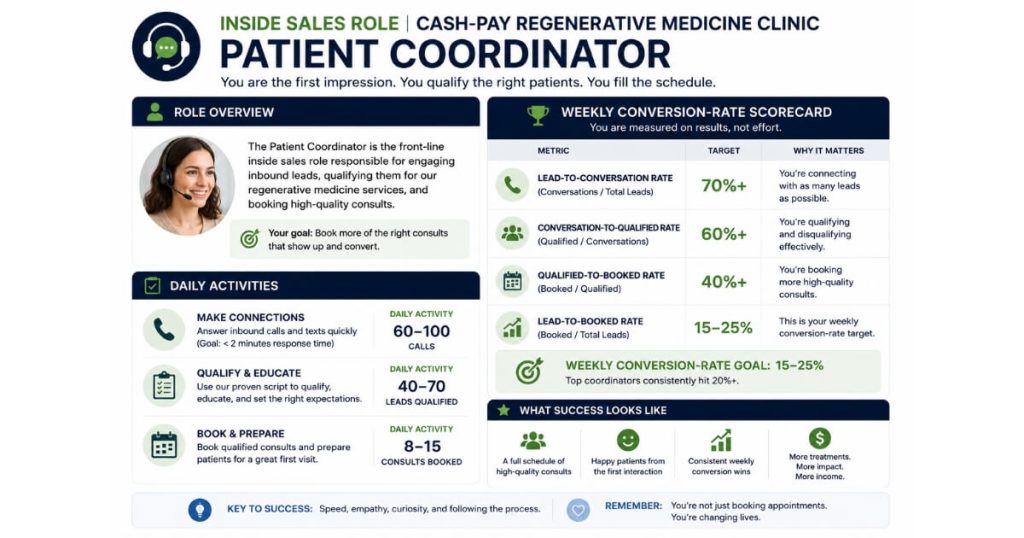
What does the inside-sales role actually look like at a cash-pay regenerative medicine clinic?
One Patient Coordinator per 200–300 monthly inquiries, dedicated to inbound leads, sitting in a phone-and-CRM seat — not the front desk.
The role is full-time.
It is not a receptionist who handles regen inquiries when the phones are quiet.
The Patient Coordinator owns every lead from:
- CRM entry
- consult booking
- procedure booking
or until the patient formally exits the funnel.
They do NOT:
- check patients in
- handle billing
- answer the general clinic line
They have one job:
Convert leads.
Daily activities
Morning
- Review every new lead from the previous evening.
- Call attempt within the first hour of the workday.
Midday
- Consult preparation calls.
- Follow-up calls for patients who consulted within the last 72 hours.
Afternoon
- Warm-list nurture.
- Follow-up with patients who said no initially.
End of day
- CRM cleanup.
- Notes on every conversation.
- Data preparation for Friday review.
Compensation
Typically:
- $50K–$65K base
- plus performance bonus
Bonus may be tied to:
- booked consults
- booked procedures
The bonus structure matters.
If paid on booked consults:
- wrong patients get booked
If paid on booked procedures:
- qualification improves
- provider calendars stay protected
How long does it take to lift a regenerative medicine clinic’s conversion rate from 20% to 60%+?
Sixty to ninety days for the first big jump.
Six months to fully stabilize the role.
Days 0–30: Setup
- Hire or reassign the Patient Coordinator.
- Write qualification script.
- Build follow-up sequence.
- Configure CRM workflows.
- Run first 100 calls to establish baseline.
Typical improvement:
- 20% → 35–40%
Days 30–60: Reps
- 200–400 calls under the new framework.
- Qualification script refinement.
- Follow-up optimization.
Typical improvement:
- Additional 15–20 points.
- 50–60% conversion range.
Days 60–90: Installation
The role becomes durable.
- Owner stops reviewing every call.
- Friday conversion-rate review becomes the key meeting.
- 70%+ conversion becomes achievable and repeatable.
The clinics that backslide do it because the owner pulls the Patient Coordinator into:
- billing
- front desk coverage
- scheduling
The 4 R’s framework only works when the role stays focused.
The pain practice down the street that does $2M in 10 months has the same lesson — a pain management practice that added $2,095,039 in revenue in 10 months on $372K of cash collected did it by protecting the inside-sales seat at all costs.
Same playbook.
Same outcome.
——————————————————————————
What’s the next step?
If you run a cash-pay regenerative medicine clinic and your lead-to-booked conversion rate is sitting at 20–30%, you do not have a marketing problem.
You have an inside-sales problem.
The fastest, highest-ROI move you can make in the next 90 days is:
- installing the Patient Coordinator role with the 4 R’s framework
The second-fastest move is auditing the four leak points and fixing them in order:
- Speed to lead
- Qualification
- Credit-card hold
- 24-hour follow-up
Most of our regen clients see conversion rate double inside 60 days.
If you want a 60-minute walk-through of where your current funnel is leaking and what your Patient Coordinator seat should look like for your specialty, book a strategy call.
We will pull your last 30 days of leads on the call and tell you the three changes that move conversion fastest.