How Should a Cash-Pay HRT Membership Clinic Rebuild Lead Conversion When New Patient Signups Stall?
The Free Discovery Call + Credit-the-Consult Playbook
Most cash-pay HRT and functional medicine membership clinics that hit a conversion wall in 2025 and 2026 are not facing a marketing problem. They’re facing a funnel-shape problem. The inbound calls are healthy. The membership pricing is competitive. But the gap between “called the clinic” and “swiped a card” got too wide as telehealth competitors moved in. Here’s the FAQ on what to change — and what not to change — when a 200-patient cash-pay HRT membership clinic suddenly gets 190 inbound calls in a month and only 12 of them sign up.
Why is my cash-pay HRT clinic getting 190 inbound calls but only 12 new member signups?
Because the gap between the first call and the provider got too wide, and prospects who already know they want TRT or peptides won’t wait through it.
When inbound volume is healthy but conversion collapses, the failure point is almost never the recurring membership price. It’s the entry point. A prospect who Googled “TRT clinic near me” or “peptide therapy” arrived already convinced they want treatment. They don’t need education. They need access. If your first ask is $900 up front for labs and a 60-minute consult before they’ve spoken to a clinician, you’re losing them to telehealth competitors who let them talk to a doctor first — for free, the same day. The math we saw at one established HRT and peptide membership clinic was stark: 190 inbound calls in a month, 12 signups. A 6% conversion rate at the bottom of a funnel that used to convert at three to four times that pace. The diagnosis wasn’t the marketing. It was the door.
Should a cash-pay HRT membership clinic accept insurance for lab work to get more signups?
No — even though the math looks attractive on a spreadsheet, insurance-paying patients are a fundamentally different avatar from cash-pay membership patients, and dropping the wall between the two dilutes both.
Cash-pay membership patients are buying access, speed, and a relationship with a clinician who has time. They stay for years and refer their family. Insurance-paying patients — in our experience at every HRT and functional medicine clinic that has tried this — typically stay three to four months, generate disproportionate admin load, and never adopt the concierge service model that makes a membership clinic profitable in the first place. The cleaner play is to offer a lighter cash-pay lab panel (around $150) for peptide-curious patients while keeping the full $550 panel for true hormone members. Protect your avatar. Don’t dilute it for a short-term conversion bump that costs more than it produces.
How do we compete with online peptide and TRT telehealth without dropping our membership price?
Compete on speed and provider access, not price. Offer a free same-day or next-day 20-minute discovery call with one of your providers as the new entry point for every inbound caller and web form.
The telehealth playbook prospects are comparing you against is a questionnaire plus a short tele-provider call, then product ships. Match that experience. Most local cash-pay clinics can’t pull this off because their providers are booked too tight or because the front desk can’t schedule on the provider’s calendar without three approvals. If your clinic has provider capacity — and most cash-pay HRT clinics under 300 patients still do — the same-day discovery call becomes your unfair advantage. The provider answers two or three real clinical questions, builds trust, and either invites the patient into the full membership lane or routes them to the peptide-only fast lane. The clinics that have moved this lever recently are seeing the conversation-to-enrollment rate climb from single digits back into the 25 to 40 percent range without changing the recurring membership price at all.

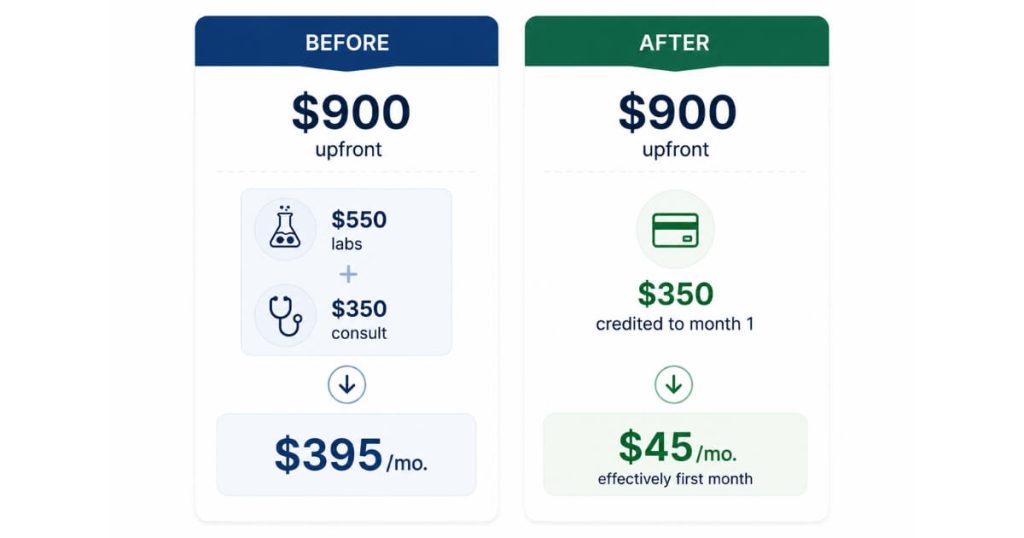
Should we credit the new-patient consult fee toward the first month of HRT membership?
Yes. Crediting the $350 consult fee toward the first month’s membership lowers the perceived up-front cost without actually cutting revenue, because prospects who sign up pay that $350 either way.
The model is borrowed from clinics that are full and turning patients away. A Sacramento-area HRT clinic we know runs $300 labs plus $300 consult credited toward the first month, then $350 per month membership — and is currently full at 220 patients with one doctor and one nurse. A clinic that scaled from 100 to 700 patients in nine months used a structurally similar credit. The math works because membership LTV — typically $4,000 to $10,000 over the life of the patient at HRT and functional medicine clinics we’ve helped scale — dwarfs the front-end “loss.” Patient acquisition cost is decoupled from front-end profitability the moment your average member stays longer than three months. Stop pricing the front door as if it has to pay for itself. Price it to convert.
Can a cash-pay HRT clinic prescribe peptides without running labs first?
Yes — there’s no legal requirement to run labs before prescribing peptides like BPC-157, tesamorelin, or AOD-9604 in a state where the clinic and provider are appropriately licensed. The discovery call plus a documented telehealth H&P is sufficient for the chart.
Build a parallel no-labs peptide lane: online questionnaire, a 20-minute tele-visit so the provider can document an H&P and SOAP note, then ship. Sell labs as the upgrade for patients who want them or want hormone work added, not as the gate that everyone has to clear before they can buy. This protects revenue from the shopper who already knows the peptide they want and would otherwise buy from a research-peptide gym counter doing six figures a month off your potential patients. It also gives you an upsell path: at the 60-day mark, when the patient trusts your providers, follow up with a discount on adding hormones. Patients who like the peptide experience adopt hormones at meaningfully higher rates than cold inbound leads do. The fast lane is also the funnel.
Should HRT providers ask new patients for the credit card, or should a separate enrollment coordinator close?
A separate enrollment coordinator should close. Providers can walk patients through pricing on the discovery call — they need to know the model cold — but the credit card and the intake forms belong to a front-office team member.
Two reasons. First, it protects the provider’s positioning as a clinician rather than a salesperson, which is exactly why the patient picked a concierge HRT membership over a CVS MinuteClinic. Second, it solves the awkwardness of a newer provider asking for $350 for an hour of their own time — a meaningful problem when a clinic is bringing in a second or third provider and revenue is suddenly tied to a junior clinician’s comfort with the close. The mechanics: the provider finishes the clinical conversation on the 20-minute call, says “I’d love to have you in the practice — I’m going to live-transfer you to Lauren, our enrollment coordinator, who will get the paperwork started,” and warm-transfers the call. The provider goes back to clinical work. The coordinator closes payment. Conversion rates rise because the two jobs aren’t tangled up.
How does a cash-pay HRT clinic recover when a star provider leaves and opens a competing clinic across town?
Expect a 15% to 20% patient dip over the following three to six months even when you see it coming, and a steady trickle of cancellation-form mentions of the departed provider for at least a year. The recovery move isn’t to chase those patients back.
It’s to rebuild the structural advantages that made them join in the first place — speed of access, a clearer entry offer, and a tighter sales conversation among the remaining providers. An HRT and peptide membership clinic we helped grow from $1M to $4M over four years saw exactly this pattern when a long-tenured provider departed and built a copycat practice across town. The fix was not to lower membership prices. It was to start recording every provider’s initial consult so the sales conversation could be audited and coached, install a free 20-minute discovery call ahead of every paid consult, and credit the consult fee to the first month of membership for everyone who enrolled. Within 90 days the conversion-to-enrollment rate from inbound calls returned to its pre-departure baseline. Don’t confuse a provider-departure loss with a pricing problem. They require different fixes.
What’s the next step?
If your cash-pay HRT or functional medicine membership clinic is sitting on a healthy inbound call volume but watching the conversion rate erode month over month — the problem is almost never your recurring membership pricing. It’s the door. The free 20-minute discovery call, the credit-the-consult model, and the two-path peptide vs. hormone funnel are the same three moves we’ve installed at multiple cash-pay HRT and concierge medicine clinics over the last twelve months to rebuild conversion without cutting the membership price. In a 60-minute strategy call we’ll audit your current new-patient funnel, calculate the conversion gap, and map the exact discovery-call + enrollment-coordinator hand-off your team needs.