How Should a Cash-Pay Women’s Hormone Clinic Position Itself to Capture the 30-Something Patient?
Most women’s hormone clinics build their entire marketing around 45+ perimenopausal and menopausal patients. They are missing the segment with the highest lifetime value and the strongest word-of-mouth — women in their early 30s whose hormonal shifts have already started and who have been told by primary care that nothing is wrong. Here’s how to position your clinic to win them.
A cash-pay women’s hormone clinic that builds its marketing exclusively around women 45+ is leaving its highest-LTV segment to the competition by default. Women in their 30s are already experiencing the cyclical hormonal shifts that drive mood swings, sleep disruption, exhausting fatigue, anxiety that comes from “nowhere,” and a quiet sense that something is off — and they are routinely told by insurance-based primary care that their labs are “normal” and to wait until they’re older. The clinic that takes their symptoms seriously and educates them clearly wins a 12–15 year patient relationship instead of a 6–8 year one. Below is the positioning, content strategy, channels, and offer structure that win the 30-something cash-pay HRT patient.
Why should a cash-pay women’s hormone clinic actively pursue patients in their 30s, not just 45+?
Because:
- 30-something women are entering hormonal shifts a full decade before most clinics start marketing to them
- they are deeply under-served by insurance-based primary care
The new clinical evidence on perimenopause is clear:
- hormonal changes start in the 30s for many women
- well before hot flashes and night sweats appear
Earlier symptoms include:
- depressed days a few times a month
- exhausted sleep that doesn’t restore
- anxiety that arrives unprovoked
- brain fog that’s “just stress”
These symptoms are:
- real
- traceable to the cyclical decline in estrogen and shifts in progesterone
…but they don’t trigger:
- the diagnostic flags primary care is trained to look for
A clinic that:
- takes these symptoms seriously
- runs comprehensive panels
- estradiol
- progesterone
- FSH
- LH
- full thyroid
- DHEA
- cortisol
…earns:
- a patient who often becomes a 12–15 year member instead of a 6–8 year member
Why?
- because she found you at 32 instead of 47
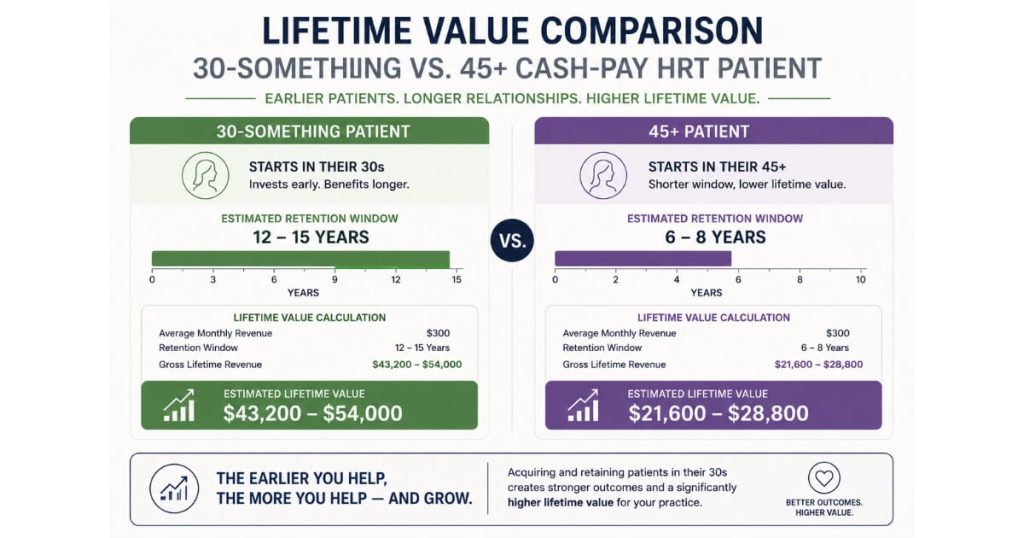
The LTV math:
- a $400/month membership over 15 years = $72,000
- versus $38,000 over 8 years
Multiply by:
- a typical referral coefficient of 1.5–2
…and the case for marketing to this segment becomes:
- overwhelming
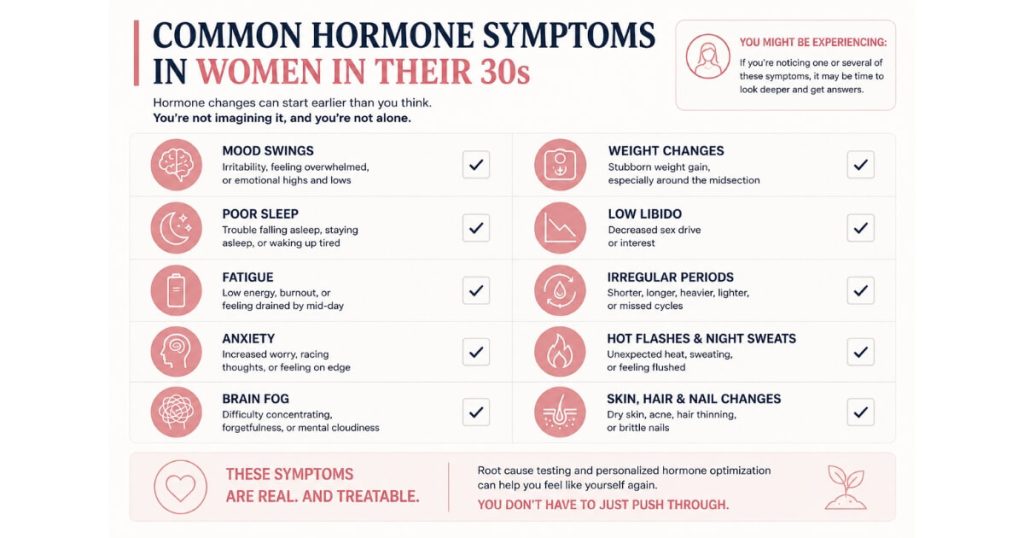
What hormonal symptoms in 30-something women are most often dismissed by primary care?
The dismissed symptoms cluster around:
- mood
- sleep
- energy
- cognition
Mood:
- depressed days a few times a month
- described as:
- “just down”
- “out of nowhere”
- often coinciding with the luteal phase
Sleep:
- trouble falling asleep
- trouble staying asleep
- waking unrefreshed
- despite no obvious stressor
Energy:
- exhausting fatigue that doesn’t make sense
- crashing after the kids’ bedtime
- no energy left for herself
Cognition:
- anxiety that arrives unprovoked
- brain fog she didn’t have at 28
- difficulty focusing on tasks she used to handle easily
Primary care often treats:
- each symptom separately
Examples:
- SSRI for mood
- sleep aid
- stimulant
- thyroid med for energy
…without looking at:
- the underlying hormonal picture
The cash-pay women’s hormone clinic that:
- runs comprehensive panels
- connects the symptoms to estradiol and progesterone cycling
…earns:
- the patient’s loyalty in a single consult
Why?
- she finally feels heard
That single moment is:
- worth thousands of dollars in LTV
How do I educate 30-something women on perimenopause without scaring them?
Lead with:
- normalizing language
- clinical curiosity
Not:
- catastrophizing
The wrong frame:
“you’re already in perimenopause and you need hormones now or your bones will deteriorate”
Why?
- that scares women out of the room
The right frame:
“what you’re experiencing is real, it’s hormonal, it’s manageable, and we have the tools to optimize how you feel without waiting until your symptoms get worse.”
Educational content should:
- explain what’s actually happening biologically
- cyclical declines in estrogen
- shifts in progesterone
- use plain language
- validate that primary care is not trained to diagnose this stage
- offer a comprehensive panel as the first step
- not a prescription
The educational hook that consistently performs best:
“Why You Don’t Feel Like Yourself at 32 — And What’s Actually Happening Hormonally.”
Publish it as:
- a long-form blog post
- a 60–90 second short-form video
- a podcast appearance
- an in-clinic handout
The piece does double duty:
- educates the patient
- pre-qualifies her for the consult
…because:
- she self-diagnoses before booking
Clinics in our portfolio that built around this content engine see:
- a meaningful increase in 30–40 patient bookings
…within:
- 60–90 days
What’s the right offer structure for a 30-something cash-pay women’s hormone patient?
The right offer for this segment is:
- a stepping-stone pricing model
Not:
- a $5,000 program
Lead with:
- a paid comprehensive consult plus full panel
- priced at $299–$599
Example:
“Comprehensive Hormone Reset Lab + Provider Review”
Why?
- low-friction first step
- tangible deliverable
- her actual labs
- explained by a provider who actually understands hormones
From there:
Transition into:
- a $300–$400/month membership
Including:
- follow-up labs
- follow-up consults
- prescribed hormones or peptides
- 15% discount on:
- supplements
- aesthetic services
The 30-something patient is:
- more skeptical of high-ticket commitments
Why?
- she has less context for what hormone optimization feels like
So:
- the stepping-stone structure converts dramatically better than a $5,000 program
The HRT clinic we scaled from $1M to $4M/year uses:
- exactly this kind of low-friction first step into a membership
…and has:
- roughly 250 active members
- at $1,000/month average
…proof that:
- the model scales when patients enter through an accessible door
Which channels work best for reaching women 30–40 for cash-pay HRT?
Highest-volume top-of-funnel channels:
- TikTok
Why?
- that’s where women 30–40 are spending attention
But:
- the content has to be educational
- not promotional
Content that performs best:
Short videos answering:
- one specific symptom question per post
Examples:
- “Why am I so anxious during my luteal phase?”
- “Why did my sleep get worse in my 30s?”
- “What’s actually happening to estrogen at 35?”
These outperform:
- branded clinic content
Why?
- they treat the viewer like an intelligent adult
- not a marketing target
Second channel:
- YouTube long-form
The same patient who watches:
- a 60-second TikTok
…will then search YouTube for:
- a 10-minute deep dive
…before booking the consult
Google Search:
- converts at a higher rate
But:
- the search volume for “hormone clinic near me” is dominated by 45+ women
To capture the 30s segment on Google:
- build a content moat around long-tail symptom queries
Examples:
- “luteal phase anxiety in 30s”
- “why can’t I sleep at 34”
- “perimenopause symptoms in early 30s”
Rank for them with:
- deeply written articles
- linked to consult booking
The same content can be repurposed as:
- podcast appearances
- downloadable PDFs
- a quarterly clinic email
Every asset:
- reinforces every other
How does an early-30s patient’s LTV compare to a 45+ patient at a women’s hormone clinic?
The early-30s patient’s LTV is:
- roughly 1.5–2× higher than the 45+ patient
…at the same membership price
The math:
At:
- $400/month average membership
A patient who joins at:
- 32
…and stays through her 50s is paying:
- $80,000–$120,000 over 17–25 years
A patient who joins at:
- 47
…and stays through her 60s is paying:
- $48,000–$72,000 over 13–18 years
The early-30s patient also has:
- higher referral coefficients
- more cross-sell potential
- peptides
- aesthetics
- weight management
- lower acquisition friction once the educational content engine is running
The catch:
- upfront patience
The 30-something patient:
- takes longer to convert
Why?
- she’s pre-qualifying herself against more competitors
- reading more content before booking
Plan for:
- a 14–30 day nurture cycle
- a CRM that doesn’t drop her at day 7
Clinics that try to convert this segment on:
- a 24-hour nurture sequence
…lose:
- 60–70% of the leads they could have closed
Clinics that nurture for:
- 30 days
…convert them and:
- keep them for 15+ years
What objections do 30-something women raise — and how do I address them in the consult?
Three objections show up repeatedly.
1. “I’m too young for hormones.”
Address by re-framing:
- optimization is not replacement
Explain:
- we’re looking at labs
- understanding her cycle
- intervening only where the data supports it
Often through:
- targeted supplementation
- lifestyle work
- low-dose protocols
Not:
- blanket HRT
2. “My doctor said my labs are normal.”
Address by showing:
- the difference between insurance-based reference ranges
- and functional reference ranges
Insurance-based ranges are:
- built around disease
Functional ranges are:
- built around how women in their 30s actually feel at their best
Walk through:
- three or four lab markers
…where the “normal” range:
- hides meaningful dysfunction
3. “I don’t want to be on something forever.”
Address by framing:
- the membership as ongoing care
- not a life sentence
Explain:
- the protocol gets reassessed every 90 days
- adjusted as symptoms and goals change
The patient maintains:
- agency the whole way
When the consult:
- covers these objections directly
- leaves the patient with her own lab results
- gives a clear next step
…close rate at this segment runs:
- 35–55%
…in our portfolio
The 30-something patient is:
- not a hard sell
She is:
- a thoughtful sell
Treat her as:
- the intelligent adult she is
Give her:
- the data
- optionality
…and she becomes:
- a 15-year member
- who tells her sister
- her best friend
- and her two coworkers