What 10 Things Must a Patient Be Clear On Before They Buy at a Cash-Pay Clinic?
A high-ticket cash-pay patient does not buy because your treatment is good.
They buy when they are clear.
Clear on their pain. Also, clear on what waiting is costing them. Clear on what their life looks like after the problem is gone. And clear that you are the person to get them there.
There are exactly ten of these clarities, and a patient who is solid on all ten says yes.
A patient who is fuzzy on even one of them asks for “more information,” says they need to talk to their spouse, or simply ghosts.
The consult is not a pitch. It is a structured conversation whose only job is to surface these ten things, in the patient’s own words, before a price is ever spoken.
This is the framework our consult teams use to turn interested callers into committed cash-pay patients.
What are the 10 things a patient must be clear on before they buy at a cash-pay clinic?
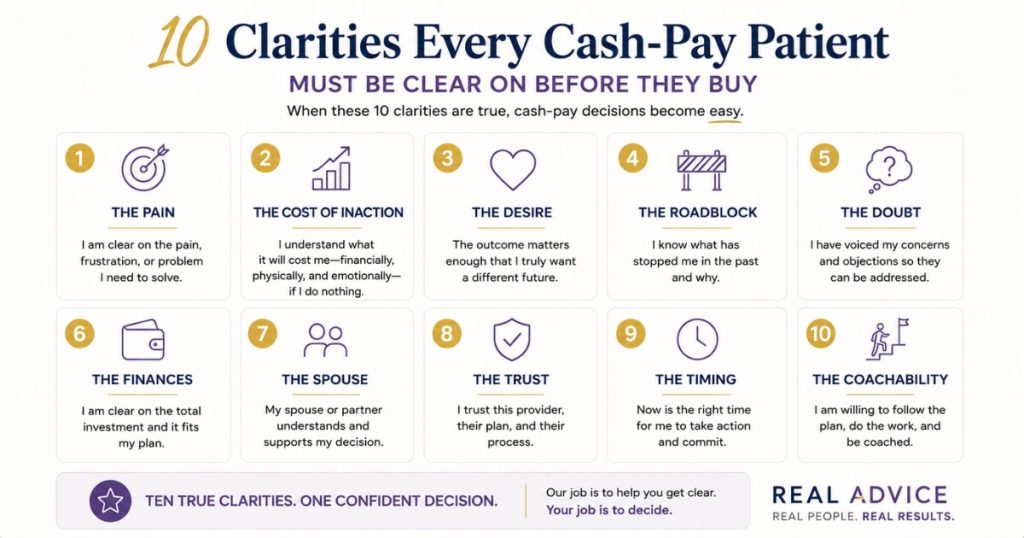
The ten clarities are:
- Their pain
- The cost of inaction versus the cost of solving it
- Their desire or goal
- The roadblock in the way
- The doubt that they can fix it on their own
- Their finances and willingness to be resourceful
- Spouse or partner alignment
- Trust
- Timing
- Coachability
Get a patient clear on all ten and they buy.
Leave any one of them fuzzy and the sale stalls.
Notice what is not on that list:
- Your credentials
- Your equipment
- Your before-and-after gallery
- Your financing terms
Those are answers to questions the patient has not yet been made to ask.
The clarities are about the patient, not about you.
A patient who is crystal clear that their problem has cost them tens of thousands of dollars and years of frustration does not haggle over price.
A patient who can picture exactly what life looks like once it is solved does not need to be pushed.
And a patient who trusts that you are the bridge to get there sees the price differently.
The price becomes obvious relative to the cost of continuing to live with the problem.
This is why a polished presentation so often loses.
Telling a patient about your service does not make them clear on their own situation.
Only questions do that.
As the framework puts it, “a doctor prescribing medicine without a proper diagnosis is malpractice.”
You diagnose first.
And the diagnosis is the ten clarities.
The same discipline sits underneath every high-converting patient acquisition system, because the best marketing in the world still dies at a consult that pitches instead of diagnoses.
How do you surface pain and the cost of inaction on the consult?
You go deeper than the surface complaint.
Then you quantify what the problem is already costing the patient.
That cost might show up in:
- Money
- Time
- Energy
- Relationships
- Quality of life
Keep going until they say the number out loud themselves.
Pain that stays vague never justifies a high-ticket cash price.
Pain that gets specific and quantified does.
The mechanics are simple, but they take discipline.
When a patient names a problem, do not jump in with, “I have just the thing for that.”
Go deeper.
Ask:
- “Can you tell me more about that?”
- “How is that showing up in your life?”
- “Who else does this affect?”
Keep an even, supportive tone.
Not hyped.
Not rushed.
A patient will not go deep with someone who is performing excitement.
Then do the math with them.
“How long has this been going on? A year? So this has cost you roughly this much. Does that sound accurate?”
Most patients have never tallied it.
When they do, the realization lands hard.
Most clients have a million-dollar problem, not a five-thousand-dollar problem.

This is the cost of inaction versus the cost of solving.
It is clarity number two, and arguably the hinge of the entire consult.
The price of your treatment has to feel small against the cost of continuing to live with the problem.
The only way to make that contrast real is to let the patient quantify the cost themselves.
This is exactly the consult discipline that turns inbound demand into closed cases.
It is the kind of system that produced 60 inbound calls a month and 250 members at Eternity Health Partners.
Marketing fills the calendar.
The cost-of-inaction conversation closes it.
How do you build desire and break the patient’s doubt and roadblocks?
You help the patient build a vivid, specific vision of life after the problem is solved.
That means the goal beyond the goal.
Then you create healthy doubt that they can reach it on their own.
Desire, roadblock, and doubt are clarities three, four, and five.
They work together.
Start with desire by asking what they want to experience instead.
Then push past the literal answer.
If they say they want more energy, ask what they would do with that energy.
Then ask what that would mean to them.
The real goal is never the treatment.
It is not even the surface outcome.
It is what that outcome creates:
- Freedom
- Confidence
- Time with family
- New choices
- A different daily life
Sell the destination, not the plane.
A patient invited to picture their new normal becomes emotionally invested in reaching it.
Then surface the roadblock and the doubt.
Ask what has stopped them from getting this on their own.
Gently challenge the belief that they can fix it themselves.
“Is this something you’re planning to handle on your own, or would you like some help with that?”
The goal is not to belittle anyone.
It is to help the patient honestly see that the way they have been approaching the problem is the same way that produced the current situation.
When a patient is clear on what they want, clear on what is in the way, and clear that going it alone has not worked, your offer becomes the obvious bridge.
Not an upsell.
How do you handle finances, spouse alignment, and trust before quoting a price?
You surface all three before the price comes up.
Not after.
Finances, spouse or partner alignment, and trust are clarities six, seven, and eight.
Every classic last-minute objection is really one of these three never having been made clear.
The objection at the end of the consult is just the bill for clarity skipped earlier.
On finances, the clarity you are after is not whether they can technically afford it.
It is whether they are willing to use the resources they have, or get resourceful.
A patient who is clear on a million-dollar problem will find five thousand dollars.
A patient still fuzzy on the cost of inaction will call any price expensive.
When the “it’s pretty expensive” objection comes, meet it with calm.
“I support whatever you decide — and it sounds like the more expensive thing to do would be to keep losing what this problem is costing you.”
On spouse or partner alignment, ask early whether anyone else is part of the decision.
Then ask how the problem affects them too.
That way, the patient can carry a confident yes home instead of a hidden no.
Trust is the broadest of the three because it has four faces:
- Trust in you
- Trust in your company
- Trust in your product
- Trust in themselves
You earn trust in you and your company by listening for what is not being said.
Then reflect the patient’s problem back more clearly than they could state it.
When you do that, they subconsciously grant you the authority to fix it.
Trust in the product comes from proof and outcomes.
Trust in themselves comes from your genuine belief that they can do this.
That blend of warmth and certainty is what scaled NuLevel Wellness Medspa to 3,727 new patients.
It was a consult experience patients trusted, not a pitch they endured.
How do you nail timing and coachability to close the consult?
You make the case for now over later.
Then you confirm the patient is willing to be guided through the process.
Timing and coachability are clarities nine and ten.
They are what convert clarity into a signed commitment.
A patient can be clear on the first eight things and still drift if “someday” stays acceptable.
They can also drift if adherence is uncertain.
On timing, the enemy is “now, later, never.”
It is the BS delay.
The soft maybe.
You make the present case real with consequence questions.
Ask:
“What’s the probable, almost-certain future if nothing changes and you keep doing exactly what you’ve been doing for the next five or ten years?”
Walk them forward.
Next month.
Next year.
Five years out.
Let them feel the accumulating cost of waiting.
Then anchor it back to now.
“What makes this a now conversation? What’s really going on?”
Timing clarity is not pressure.
It is helping the patient see that the cost of waiting compounds.
Coachability is the final filter.
You can only help a patient to the degree they are willing to help themselves.
So you test, gently, whether they will follow the protocol and do their part.
A patient who wants the result but resists every instruction is a refund and a bad review waiting to happen.
A coachable patient clear on the other nine clarities is your highest-LTV, most-referring patient.
When all ten are in place, you do not have to close hard.
You simply ask where they would like to go from here.
And the patient closes themselves.
As Dale Carnegie put it, “a man convinced against his will is of the same opinion still.”
That is exactly why the ten clarities convince the patient with their own words instead of yours.
FAQ’s About the 10 Clarities Before a Patient Buys
What are the 10 things a patient must be clear on before they buy at a cash-pay clinic?
The 10 clarities are:
- Their pain
- The cost of inaction versus the cost of solving it
- Their desire or goal
- The roadblock in the way
- The doubt that they cannot fix it on their own
- Their finances and willingness to be resourceful
- Their spouse or partner alignment
- Trust in you, your company, your product, and themselves
- Timing
- Coachability
A patient who is clear on all ten will buy.
A patient who is fuzzy on any one of them will stall, ask for more information, or ghost.
The consult is not a presentation of your service.
It is a structured conversation that surfaces each of these ten things, in the patient’s own words, before you ever quote a price.
Most clinics lose the sale not because the patient could not afford the treatment.
They lose because the patient was never made clear on the pain, the cost of waiting, or what their life looks like after the problem is solved.
When a patient hears their own situation reflected back more clearly than they could articulate it themselves, they subconsciously grant you the authority to fix it.
That is the entire job of the consult.
Why do cash-pay patients ask for more information instead of buying?
Because asking for more information is almost never about information.
It is a polite way to delay a decision they are scared to make.
When a patient says, “I just want some info on what you do,” that is a trap.
Falling for it kills the sale.
They are vague because they have not been made clear on their own pain, the cost of waiting, or what solving the problem creates for them.
The fix is not to hand over more facts.
It is to gently redirect them back to the problem with a question like:
“I’d love to tell you about that — and let me ask you, why is that important to you right now?”
When they go vague and general, you get specific, deep, and meaningful.
Clarity on the ten things is what moves a cash-pay patient from interested to committed.
- Not more brochures.
- Not more before-and-after photos.
- Not more pricing PDFs.
How do you surface the cost of inaction on a cash-pay consult?
You quantify what the problem is already costing the patient.
That cost may show up in money, time, energy, relationships, or quality of life.
Keep going until they say the number out loud themselves.
Most patients have a million-dollar problem, not a five-thousand-dollar problem.
They just have not done the math.
You help them do it.
“How long has this been going on? A year? So this has cost you roughly this much — does that sound accurate?”
The point is not to manipulate.
It is to help them get clear.
The cost of inaction must feel larger than the price of the treatment, or the price will always feel expensive.
Real ADvice teaches clinic consult teams to frame the offer as the cost of solving versus the far greater cost of continuing to live with the problem.
That contrast, surfaced in the patient’s own words, is what makes a high-ticket cash price feel like the obvious choice.
Should you handle the spouse or partner objection during the consult?
Yes.
Spouse or partner alignment is one of the ten clarities.
You surface it before you quote the price, not after.
“I need to talk to my partner” at the end of a consult is usually a stall dressed up as diligence.
It happens because the patient was never made clear enough on the pain and the desired outcome to advocate for the decision themselves.
Ask early whether anyone else is part of this decision.
Then ask how the problem is affecting them too.
If the partner is affected by the same problem — the patient’s energy, mood, confidence, or health — bring that into the conversation.
That way, the patient can carry the case home with conviction.
When all ten clarities are in place, the spouse conversation becomes a shared yes instead of a hidden no.
What does coachability mean in a cash-pay sales consult, and why does it matter?
Coachability is the patient’s willingness to follow the protocol, do their part, and be guided through the process.
It is the tenth clarity because you can only help a patient to the degree they are willing to help themselves.
A patient who wants the result but resists every instruction is not a buyer you want.
The outcome depends on adherence.
On the consult, test for it gently.
Ask yourself:
- Are they answering honestly?
- Are they open to seeing the problem differently?
- Do they accept that the way they have been thinking about it has produced their current situation?
A coachable patient who is clear on the other nine things is your best long-term, highest-LTV patient.
Screening for coachability protects your outcomes, your reviews, and your reputation.
How is the 10 clarities framework different from a normal sales script?
A normal sales script tells the patient about the product.
The 10 clarities framework uses questions to help the patient get clear about themselves.
The principle is simple:
“Selling is not telling — questions are the answer.”
And:
“A doctor prescribing medicine without a proper diagnosis is malpractice.”
You diagnose before you demonstrate.
Instead of pitching the treatment, you move through problem, vision, and consequence questions.
You do that until the patient is clear on all ten things.
Only then do you present the offer as the bridge between where they are and where they want to be.
It is patient-centered, not product-centered.
That is why it converts high-ticket cash offers that a pushy pitch would lose.
It is the same consult discipline behind the patient-acquisition systems Real ADvice builds for cash-pay clinics.